

Stepped osteotomy of femoral head autograft for acetabular reconstruction in total hip arthroplasty for dysplasia of the hip: 3 to 12 years' results
- PMID: 32584737
- PMCID: PMC7489182
- DOI: 10.5606/ehc.2020.74300
Stepped osteotomy of femoral head autograft for acetabular reconstruction in total hip arthroplasty for dysplasia of the hip: 3 to 12 years' results
Abstract
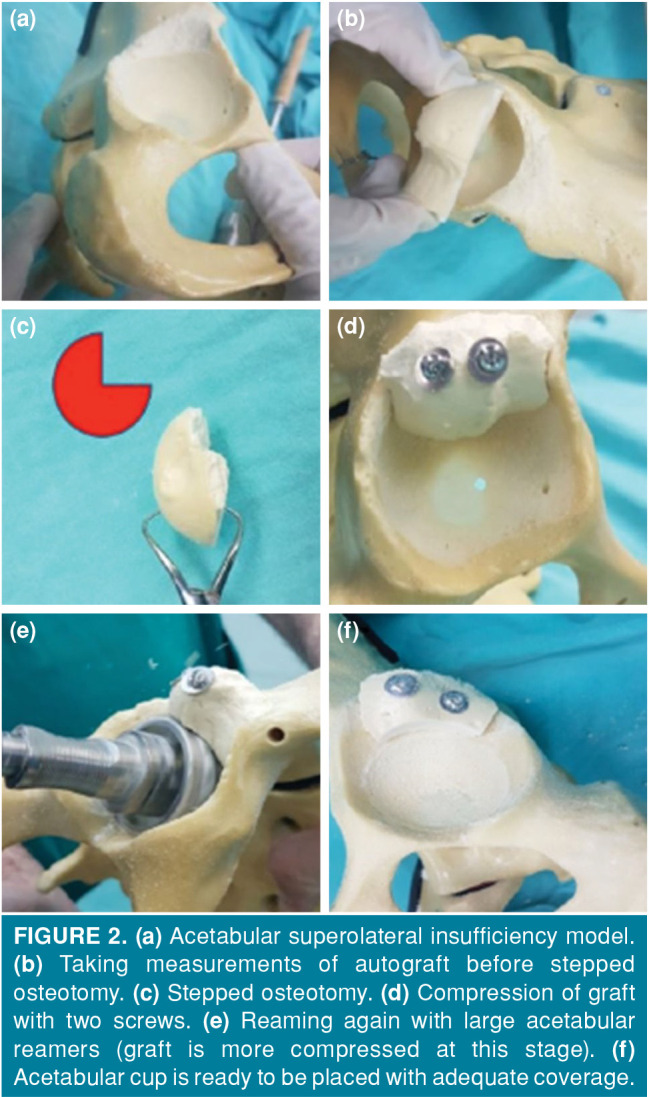
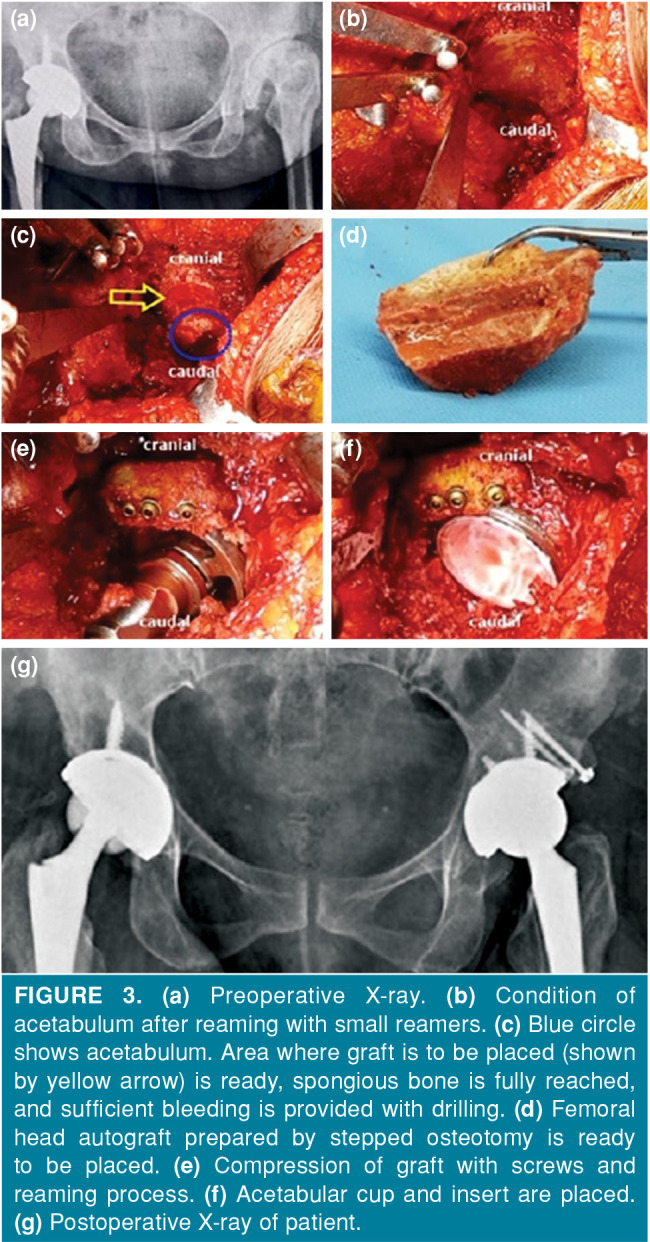
Objectives: This study aims to describe a stepped osteotomy technique applied to the femoral head autograft to keep the graft volume at a sufficient level, provide primary stability, and direct cancellous-cancellous bone contact.
Patients and methods: In this retrospective study, 24 hips of 20 patients (5 males, 15 females; mean age 53 years; range, 43 to 68 years) with dysplasia of the hip (DDH) who underwent total hip arthroplasty with femoral head stepped osteotomy technique were evaluated between April 2003 and June 2010. Patients' age, gender, operation side, and postoperative complications were recorded. Aseptic loosening of the acetabular cup and graft integration/resorption were evaluated radiographically. Radiological evaluations were performed according to the methods of DeLee and Charnley, and Mulroy and Harris. Functional status of the patients was determined according to the criteria of Merle d'Aubigné and Postel, and Harris hip score (HHS).
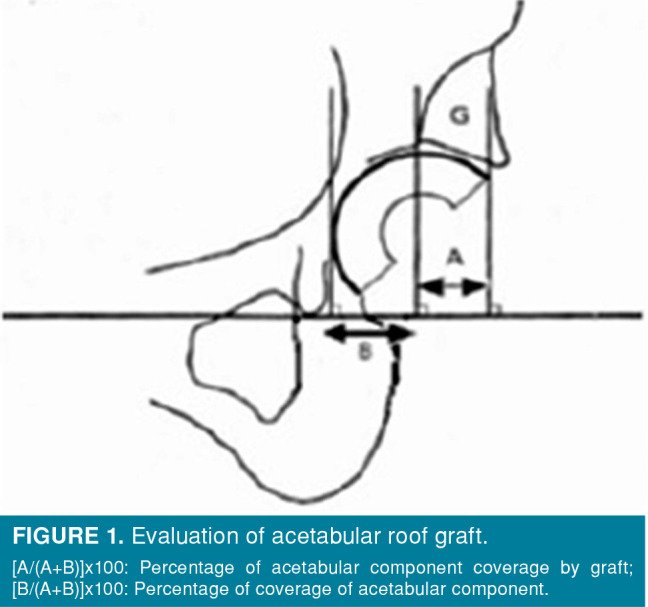
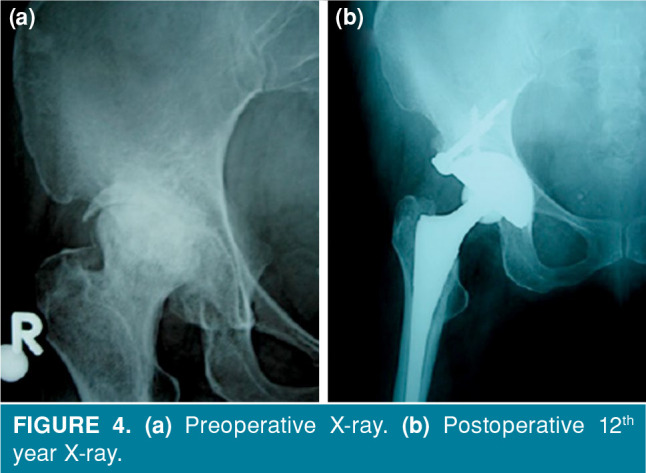
Results: The mean follow-up period was 5.5 years (range, 3 to 12 years). None of the patients had any complications in the early postoperative period. In all patients, the percentage of acetabular component coverage by the graft was measured as 27% (range, 19 to 38%) on average. At the last follow-up, all patients were satisfied with the result and there was no sign of clinically loosening, osteointegration was complete, and there was no radiographic evidence of graft resorption or collapse of any hip. The overall Merle d'Aubigné scores and HHSs of the patients significantly improved at the final follow-up.
Conclusion: This stepped osteotomy technique increases the probability of osteointegration, reduces the need for early revision, and provides reliable stability with satisfactory clinical and radiological midterm results.
Conflict of interest statement
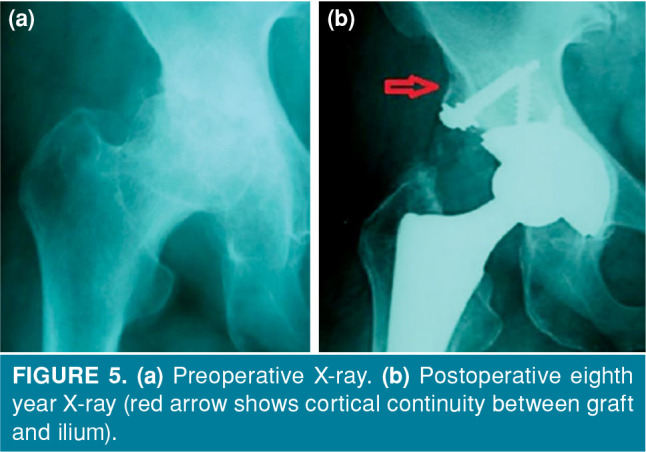
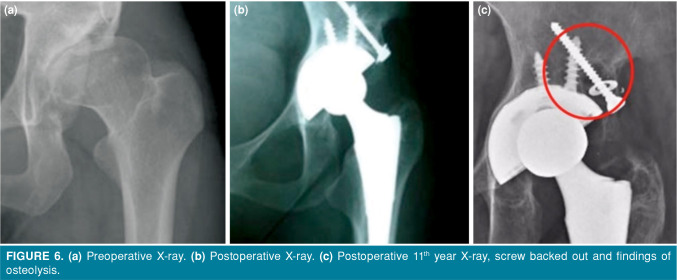
Figures
References
-
- Harris WH, Crothers O, Oh I. Total hip replacement and femoral-head bone-grafting for severe acetabular deficiency in adults. J Bone Joint Surg [Am] 1977;59:752–759. - PubMed
-
- Gerber SD, Harris WH. Femoral head autografting to augment acetabular deficiency in patients requiring total hip replacement. A minimum five-year and an average seven-year follow-up study. J Bone Joint Surg [Am] 1986;68:1241–1248. - PubMed
-
- Shinar AA, Harris WH. Bulk structural autogenous grafts and allografts for reconstruction of the acetabulum in total hip arthroplasty. Sixteen-year-average follow-up J Bone Joint Surg [Am] 1997;79:159–168. - PubMed
-
- Iida H, Matsusue Y, Kawanabe K, Okumura H, Yamamuro T, Nakamura T. Cemented Total Hip Arthroplasty With Acetabular Bone Graft for Developmental Dysplasia. Long- term Results and Survivorship Analysis. J Bone Joint Surg [Br] 2000;82:176–184. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
