

Machine learning insight into the role of imaging and clinical variables for the prediction of obstructive coronary artery disease and revascularization: An exploratory analysis of the CONSERVE study
- PMID: 32584909
- PMCID: PMC7316297
- DOI: 10.1371/journal.pone.0233791
Machine learning insight into the role of imaging and clinical variables for the prediction of obstructive coronary artery disease and revascularization: An exploratory analysis of the CONSERVE study
Abstract
Background: Machine learning (ML) is able to extract patterns and develop algorithms to construct data-driven models. We use ML models to gain insight into the relative importance of variables to predict obstructive coronary artery disease (CAD) using the Coronary Computed Tomographic Angiography for Selective Cardiac Catheterization (CONSERVE) study, as well as to compare prediction of obstructive CAD to the CAD consortium clinical score (CAD2). We further perform ML analysis to gain insight into the role of imaging and clinical variables for revascularization.
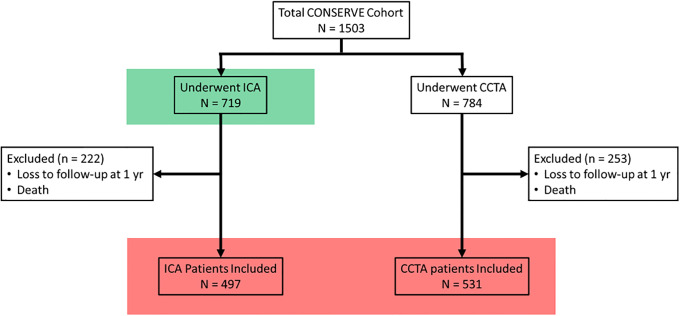
Methods: For prediction of obstructive CAD, the entire ICA arm of the study, comprising 719 patients was used. For revascularization, 1,028 patients were randomized to invasive coronary angiography (ICA) or coronary computed tomographic angiography (CCTA). Data was randomly split into 80% training 20% test sets for building and validation. Models used extreme gradient boosting (XGBoost).
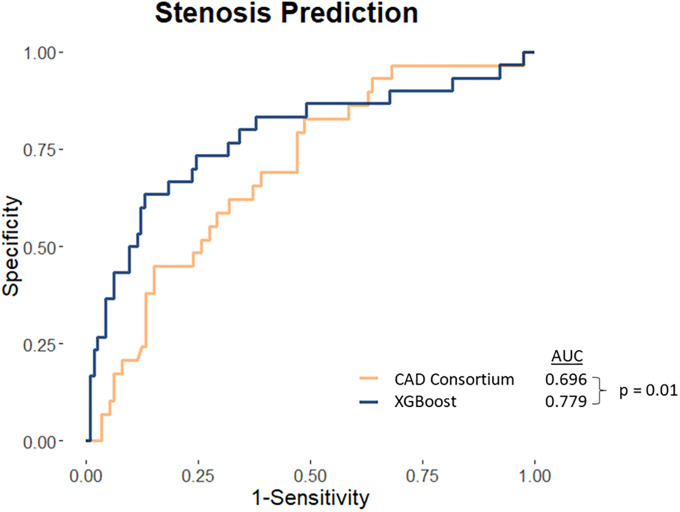
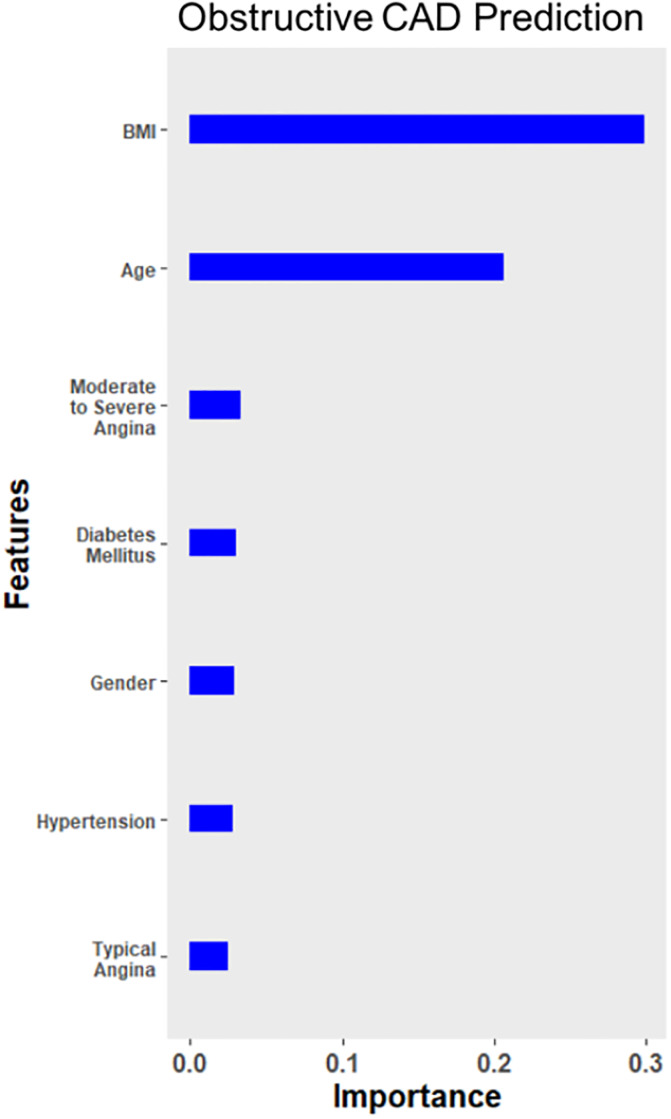
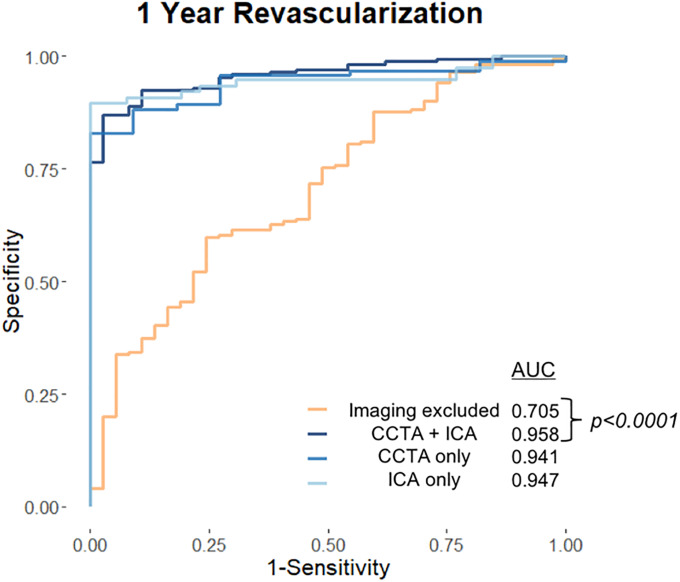
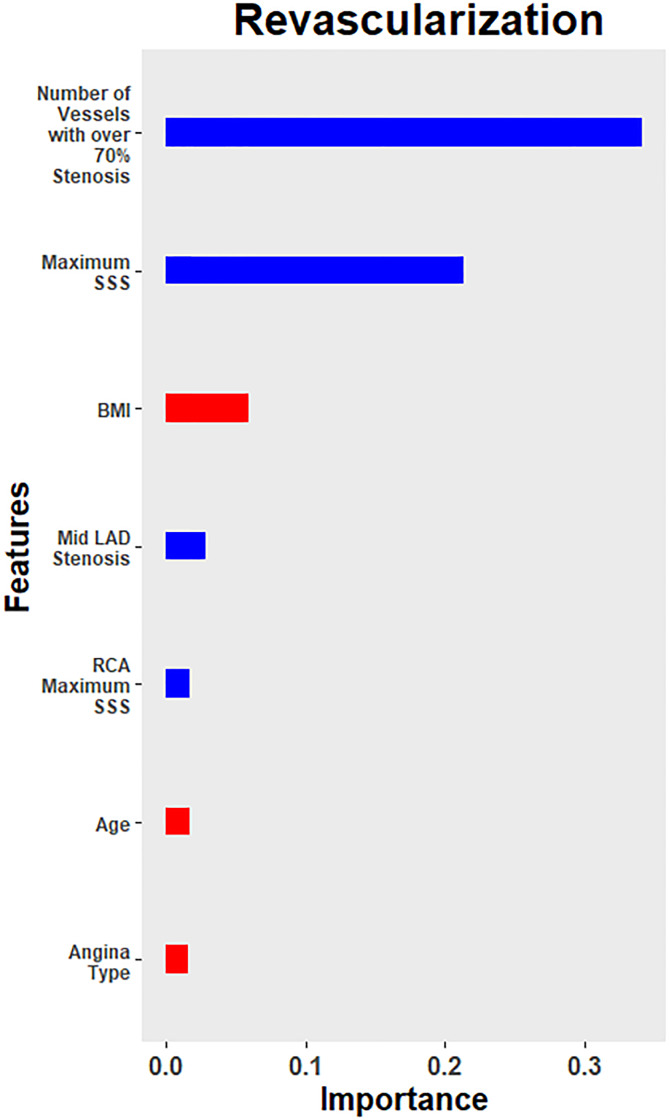
Results: Mean age was 60.6 ± 11.5 years and 64.3% were female. For the prediction of obstructive CAD, the AUC was significantly higher for ML at 0.779 (95% CI: 0.672-0.886) than for CAD2 (0.696 [95% CI: 0.594-0.798]) (P = 0.01). BMI, age, and angina severity were the most important variables. For revascularization, the model obtained an overall area under the receiver-operation curve (AUC) of 0.958 (95% CI = 0.933-0.983). Performance did not differ whether the imaging parameters used were from ICA (AUC 0.947, 95% CI = 0.903-0.990) or CCTA (AUC 0.941, 95% CI = 0.895-0.988) (P = 0.90). The ML model obtained sensitivity and specificity of 89.2% and 92.9%, respectively. Number of vessels with ≥70% stenosis, maximum segment stenosis severity (SSS) and body mass index (BMI) were the most important variables. Exclusion of imaging variables resulted in performance deterioration, with an AUC of 0.705 (95% CI 0.614-0.795) (P <0.0001).
Conclusions: For obstructive CAD, the ML model outperformed CAD2. BMI is an important variable, although currently not included in most scores. In this ML model, imaging variables were most associated with revascularization. Imaging modality did not influence model performance. Removal of imaging variables reduced model performance.
Conflict of interest statement
The authors have read the journal's policy and the authors of this paper have the following competing interests: James K. Min is founder, paid employee, and has equity interest in Cleerly Health. However, he was an employee of the Dalio Institute of Cardiovascular Imaging at the time of the study. James K. Min also serves on the scientific advisory board of Arineta and GE Healthcare. Leslee Shaw has an equity interest in Cleerly Health. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose. There are no patents, products in development or marketed products associated with this research to declare. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Douglas PS, Patel MR, Bailey SR, Dai D, Kaltenbach L, Brindis RG, et al. Hospital Variability in the Rate of Finding Obstructive Coronary Artery Disease at Elective, Diagnostic Coronary Angiography. Journal of the American College of Cardiology. 2011;58(8):801–809. 10.1016/j.jacc.2011.05.019 - DOI - PubMed
-
- Patel MR, Dai D, Hernandez AF, Douglas PS, Messenger J, Garratt KN, et al. Prevalence and predictors of nonobstructive coronary artery disease identified with coronary angiography in contemporary clinical practice. American Heart Journal. 2014;167(6):846–852.e2. 10.1016/j.ahj.2014.03.001 - DOI - PubMed
-
- Patel MR, Bailey SR, Bonow RO, Chambers CE, Chan PS, Dehmer GJ, et al. ACCF/SCAI/AATS/AHA/ASE/ASNC/HFSA/HRS/SCCM/SCCT/SCMR/STS 2012 appropriate use criteria for diagnostic catheterization: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, Society for Cardiovascular Angiography and Interventions, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society of Critical Care Medicine, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2012;59(22):1995–2027. 10.1016/j.jacc.2012.03.003 - DOI - PubMed
-
- Budoff MJ, Dowe D, Jollis JG, Gitter M, Sutherland J, Halamert E, et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol. 2008;52(21):1724–1732. 10.1016/j.jacc.2008.07.031 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
