

Development and validation of a robotic multifactorial fall-risk predictive model: A one-year prospective study in community-dwelling older adults
- PMID: 32584912
- PMCID: PMC7316263
- DOI: 10.1371/journal.pone.0234904
Development and validation of a robotic multifactorial fall-risk predictive model: A one-year prospective study in community-dwelling older adults
Abstract
Background: Falls in the elderly are a major public health concern because of their high incidence, the involvement of many risk factors, the considerable post-fall morbidity and mortality, and the health-related and social costs. Given that many falls are preventable, the early identification of older adults at risk of falling is crucial in order to develop tailored interventions to prevent such falls. To date, however, the fall-risk assessment tools currently used in the elderly have not shown sufficiently high predictive validity to distinguish between subjects at high and low fall risk. Consequently, predicting the risk of falling remains an unsolved issue in geriatric medicine. This one-year prospective study aims to develop and validate, by means of a cross-validation method, a multifactorial fall-risk model based on clinical and robotic parameters in older adults.
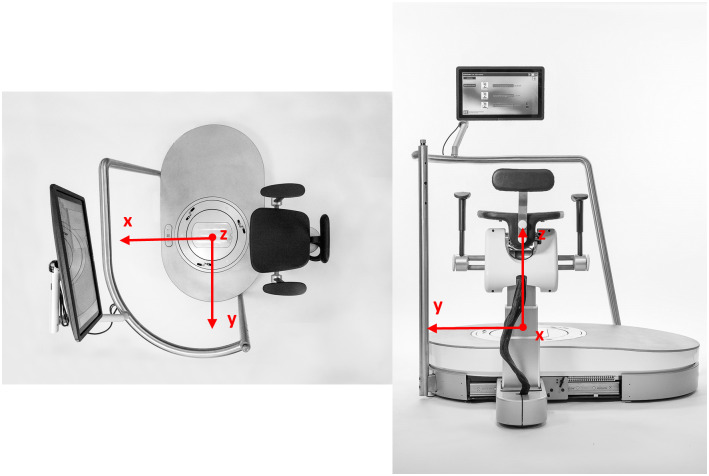
Methods: Community-dwelling subjects aged ≥ 65 years were enrolled. At the baseline, all subjects were evaluated for history of falling and number of drugs taken daily, and their gait and balance were evaluated by means of the Timed "Up & Go" test (TUG), Gait Speed (GS), Short Physical Performance Battery (SPPB) and Performance-Oriented Mobility Assessment (POMA). They also underwent robotic assessment by means of the hunova robotic device to evaluate the various components of balance. All subjects were followed up for one-year and the number of falls was recorded. The models that best predicted falls-on the basis of: i) only clinical parameters; ii) only robotic parameters; iii) clinical plus robotic parameters-were identified by means of a cross-validation method.
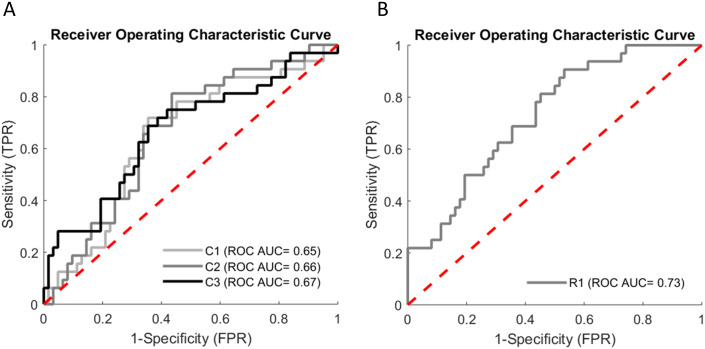
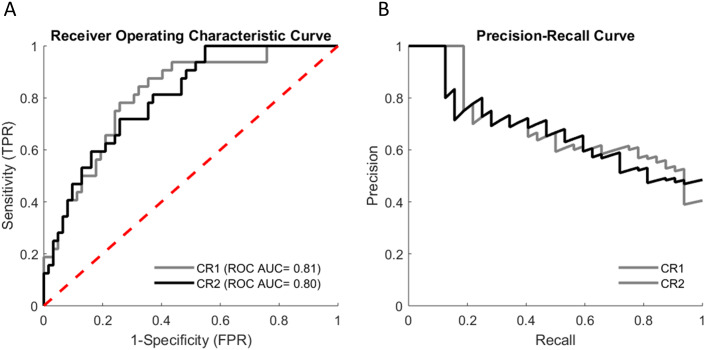
Results: Of the 100 subjects initially enrolled, 96 (62 females, mean age 77.17±.49 years) completed the follow-up and were included. Within one year, 32 participants (33%) experienced at least one fall ("fallers"), while 64 (67%) did not ("non-fallers"). The best classifier model to emerge from cross-validated fall-risk estimation included eight clinical variables (age, sex, history of falling in the previous 12 months, TUG, Tinetti, SPPB, Low GS, number of drugs) and 20 robotic parameters, and displayed an area under the receiver operator characteristic (ROC) curve of 0.81 (95% CI: 0.72-0.90). Notably, the model that included only three of these clinical variables (age, history of falls and low GS) plus the robotic parameters showed similar accuracy (ROC AUC 0.80, 95% CI: 0.71-0.89). In comparison with the best classifier model that comprised only clinical parameters (ROC AUC: 0.67; 95% CI: 0.55-0.79), both models performed better in predicting fall risk, with an estimated Net Reclassification Improvement (NRI) of 0.30 and 0.31 (p = 0.02), respectively, and an estimated Integrated Discrimination Improvement (IDI) of 0.32 and 0.27 (p<0.001), respectively. The best model that comprised only robotic parameters (the 20 parameters identified in the final model) achieved a better performance than the clinical parameters alone, but worse than the combination of both clinical and robotic variables (ROC AUC: 0.73, 95% CI 0.63-0.83).
Conclusion: A multifactorial fall-risk assessment that includes clinical and hunova robotic variables significantly improves the accuracy of predicting the risk of falling in community-dwelling older people. Our data suggest that combining clinical and robotic assessments can more accurately identify older people at high risk of falls, thereby enabling personalized fall-prevention interventions to be undertaken.
Conflict of interest statement
A.D.L., V.S., J.S. and C.S. are employees of Movendo Technology (Genova, Italy). S.P. is a consultant for Movendo Technology (Genova, Italy). This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
The Aachen Mobility and Balance Index to measure physiological falls risk: a comparison with the Tinetti POMA Scale.Eur J Trauma Emerg Surg. 2016 Oct;42(5):537-545. doi: 10.1007/s00068-016-0693-2. Epub 2016 Jun 10. Eur J Trauma Emerg Surg. 2016. PMID: 27287271
-
Evaluating the discriminatory power of the velocity field diagram and timed-up-and-go test in determining the fall status of community-dwelling older adults: a cross-sectional observational study.BMC Geriatr. 2022 Aug 11;22(1):658. doi: 10.1186/s12877-022-03282-2. BMC Geriatr. 2022. PMID: 35948869 Free PMC article.
-
Four Months of Wearing a Balance Orthotic Improves Measures of Balance and Mobility Among a Cohort of Community-Living Older Adults.J Geriatr Phys Ther. 2019 Oct/Dec;42(4):216-223. doi: 10.1519/JPT.0000000000000174. J Geriatr Phys Ther. 2019. PMID: 29351127 Clinical Trial.
-
Functional Reach Test, Single-Leg Stance Test, and Tinetti Performance-Oriented Mobility Assessment for the Prediction of Falls in Older Adults: A Systematic Review.Phys Ther. 2021 Oct 1;101(10):pzab173. doi: 10.1093/ptj/pzab173. Phys Ther. 2021. PMID: 34244801
-
Exercise for preventing falls in older people living in the community.Cochrane Database Syst Rev. 2019 Jan 31;1(1):CD012424. doi: 10.1002/14651858.CD012424.pub2. Cochrane Database Syst Rev. 2019. PMID: 30703272 Free PMC article.
Cited by
-
Standard versus innovative robotic balance assessment for people with multiple sclerosis: a correlational study.Eur J Med Res. 2023 Jul 26;28(1):254. doi: 10.1186/s40001-023-01223-2. Eur J Med Res. 2023. PMID: 37491303 Free PMC article.
-
Biomechanical analysis of limits of stability using computerized posturography: correlations with functional mobility in elderly individuals with hip osteoarthritis - a cross-sectional study.Front Bioeng Biotechnol. 2024 Nov 25;12:1440393. doi: 10.3389/fbioe.2024.1440393. eCollection 2024. Front Bioeng Biotechnol. 2024. PMID: 39654827 Free PMC article.
-
Evaluation of a novel technology-supported fall prevention intervention - study protocol of a multi-centre randomised controlled trial in older adults at increased risk of falls.BMC Geriatr. 2023 Feb 18;23(1):103. doi: 10.1186/s12877-023-03810-8. BMC Geriatr. 2023. PMID: 36803459 Free PMC article.
-
Comparing Machine Learning Methods to Improve Fall Risk Detection in Elderly with Osteoporosis from Balance Data.J Healthc Eng. 2021 Sep 9;2021:8697805. doi: 10.1155/2021/8697805. eCollection 2021. J Healthc Eng. 2021. PMID: 34540190 Free PMC article.
-
Escalating Risks: Injury Patterns in Escalator-Related Trauma.Cureus. 2024 Nov 26;16(11):e74535. doi: 10.7759/cureus.74535. eCollection 2024 Nov. Cureus. 2024. PMID: 39735070 Free PMC article.
References
-
- World Health Organization (2018). Fact sheet: Falls. https://www.who.int/news-room/fact-sheets/detail/falls. Accessed February 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
