

Withdrawal of Life-supporting Treatment in Severe Traumatic Brain Injury
- PMID: 32584926
- PMCID: PMC7301301
- DOI: 10.1001/jamasurg.2020.1790
Withdrawal of Life-supporting Treatment in Severe Traumatic Brain Injury
Abstract
Importance: There are limited data on which factors affect the critical and complex decision to withdraw life-supporting treatment (LST) in patients with severe traumatic brain injury (sTBI).
Objective: To determine demographic and clinical factors associated with the decision to withdraw LST in patients with sTBI.
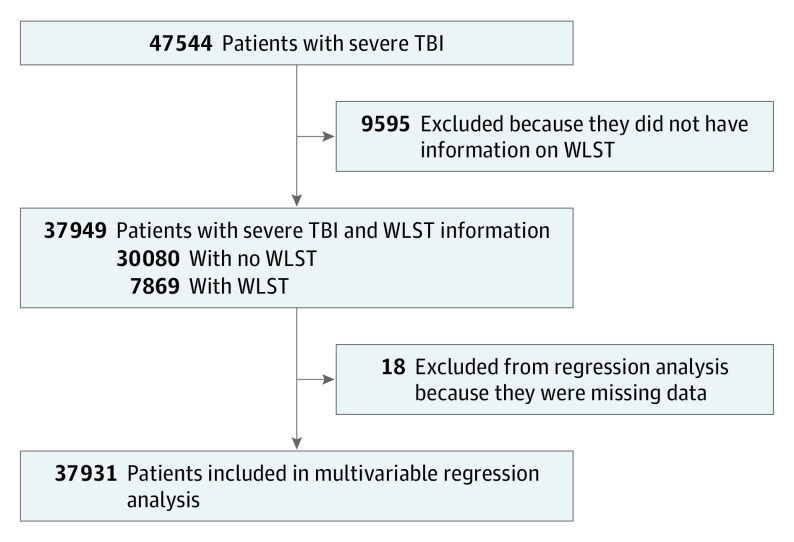
Design, setting, and participants: This retrospective analysis of inpatient data from more than 825 trauma centers across the US in the American College of Surgeons Trauma Quality Improvement Program database from January 2013 to December 2015 included adult patients with sTBI and documentation of a decision regarding withdrawal of LST (WLST). Data analysis was conducted in September 2019.
Main outcomes and measures: Factors associated with WLST in sTBI.
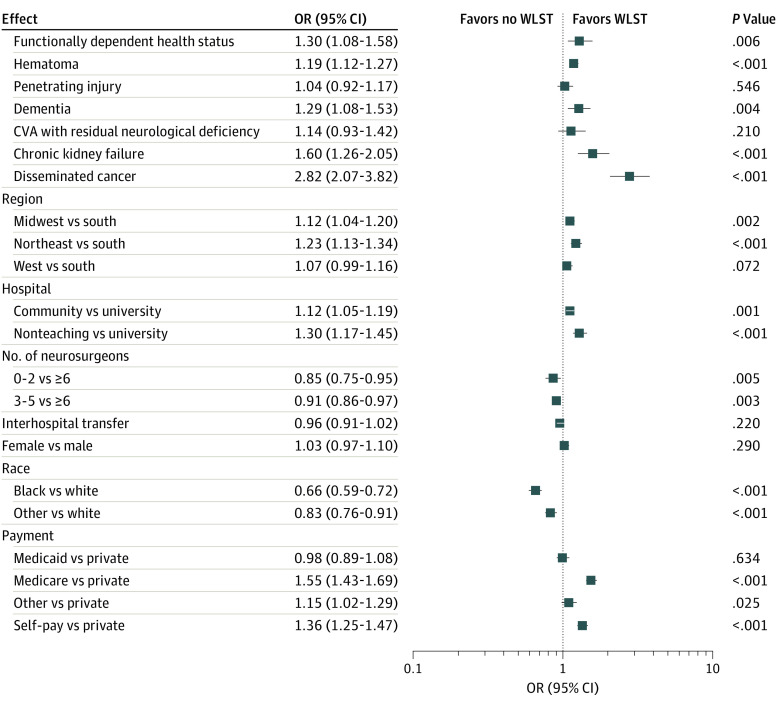
Results: A total of 37931 patients (9817 women [25.9%]) were included in the multivariable analysis; 7864 (20.7%) had WLST. Black patients (4806 [13.2%]; odds ratio [OR], 0.66; 95% CI, 0.59-0.72; P < .001) and patients of other race (4798 [13.2%]; OR, 0.83; 95% CI, 0.76-0.91; P < .001) were less likely than white patients (26 864 [73.7%]) to have WLST. Patients from hospitals in the Midwest (OR, 1.12; 95% CI, 1.04-1.20; P = .002) or Northeast (OR, 1.23; 95% CI, 1.13-1.34; P < .001) were more likely to have WLST than patients from hospitals in the South. Patients with Medicare (OR, 1.55; 95% CI, 1.43-1.69; P < .001) and self-pay patients (OR, 1.36; 95% CI, 1.25-1.47; P < .001) were more likely to have WLST than patients with private insurance. Older patients and those with lower Glasgow Coma Scale scores, higher Injury Severity Scores, or craniotomy were generally more likely to have WLST. Withdrawal of LST was more likely for patients with functionally dependent health status (OR, 1.30; 95% CI, 1.08-1.58; P = .01), hematoma (OR, 1.19; 95% CI, 1.12-1.27; P < .001), dementia (OR, 1.29; 95% CI, 1.08-1.53; P = .004), and disseminated cancer (OR, 2.82; 95% CI, 2.07-3.82; P < .001) than for patients without these conditions.
Conclusions and relevance: Withdrawal of LST is common in sTBI and socioeconomic factors are associated with the decision to withdraw LST. These results highlight the many factors that contribute to decision-making in sTBI and demonstrate that in a complex and variable disease process, variation based on race, payment, and region presents as a potential challenge.
Conflict of interest statement
Figures
Comment in
-
Dying of Traumatic Brain Injury-Palliative Care too Soon, or too Late?JAMA Surg. 2020 Aug 1;155(8):731. doi: 10.1001/jamasurg.2020.1810. JAMA Surg. 2020. PMID: 32584939 No abstract available.
References
-
- Turgeon AF, Lauzier F, Burns KEA, et al. ; Canadian Critical Care Trials Group . Determination of neurologic prognosis and clinical decision making in adult patients with severe traumatic brain injury: a survey of Canadian intensivists, neurosurgeons, and neurologists. Crit Care Med. 2013;41(4):1086-1093. doi: 10.1097/CCM.0b013e318275d046 - DOI - PubMed
-
- Finkelstein E, Corso PS, Miller TR. The Incidence and Economic Burden of Injuries in the United States. Oxford University Press; 2006. doi: 10.1093/acprof:oso/9780195179484.001.0001 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
