

Association of the Placement of a Perirectal Hydrogel Spacer With the Clinical Outcomes of Men Receiving Radiotherapy for Prostate Cancer: A Systematic Review and Meta-analysis
- PMID: 32585020
- PMCID: PMC7301230
- DOI: 10.1001/jamanetworkopen.2020.8221
Association of the Placement of a Perirectal Hydrogel Spacer With the Clinical Outcomes of Men Receiving Radiotherapy for Prostate Cancer: A Systematic Review and Meta-analysis
Abstract
Importance: Perirectal spacers are intended to lower the risk of rectal toxic effects associated with prostate radiotherapy. A quantitative synthesis of typical clinical results with specific perirectal spacers is limited.
Objective: To evaluate the association between perirectal hydrogel spacer placement and clinical outcomes of men receiving radiotherapy for prostate cancer.
Data sources: A systematic search was performed of the Cochrane Central Register of Controlled Trials, MEDLINE, and Embase for articles published through September 2019.
Study selection: Studies comparing men who received a hydrogel spacer vs men who did not receive a spacer (controls) prior to prostate radiotherapy.
Data extraction and synthesis: Via random-effects meta-analysis, group comparisons were reported using the weighted mean difference for continuous measures and the risk ratio for binary measures.
Main outcomes and measures: Procedural results, the percentage volume of rectum receiving at least 70 Gy radiation (v70), early (≤3 months) and late (>3 months) rectal toxic effects, and early and late changes in bowel-related quality of life on the Expanded Prostate Cancer Index Composite (minimal clinically important difference, 4 points).
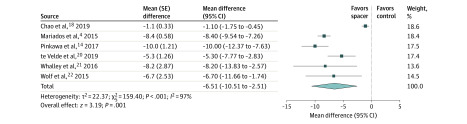
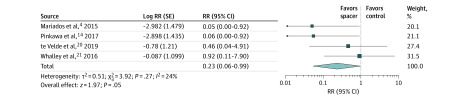
Results: The review included 7 studies (1 randomized clinical trial and 6 cohort studies) involving 1011 men (486 who received a hydrogel spacer and 525 controls), with a median duration of patient follow-up of 26 months (range, 3-63 months). The success rate of hydrogel spacer placement was 97.0% (95% CI, 94.4%-98.8% [5 studies]), and the weighted mean perirectal separation distance was 11.2 mm (95% CI, 10.1-12.3 mm [5 studies]). Procedural complications were mild and transient, occurring in 0% to 10% of patients within the studies. The hydrogel spacer group received 66% less v70 rectal irradiation compared with controls (3.5% vs 10.4%; mean difference, -6.5%; 95% CI, -10.5% to -2.5%; P = .001 [6 studies]). The risk of grade 2 or higher rectal toxic effects was comparable between groups in early follow-up (4.5% in hydrogel spacer group vs 4.1% in control group; risk ratio, 0.82; 95% CI, 0.52-1.28; P = .38 [6 studies]) but was 77% lower in the hydrogel spacer group in late follow-up (1.5% vs 5.7%; risk ratio, 0.23; 95% CI, 0.06-0.99; P = .05 [4 studies]). Changes in bowel-related quality of life were comparable between groups in early follow-up (mean difference, 0.2; 95% CI, -3.1 to 3.4; P = .92 [2 studies]) but were greater in the hydrogel spacer group in late follow-up (mean difference, 5.4; 95% CI, 2.8-8.0; P < .001 [2 studies]).
Conclusions and relevance: For men receiving prostate radiotherapy, injection of a hydrogel spacer was safe, provided prostate-rectum separation sufficient to reduce v70 rectal irradiation, and was associated with fewer rectal toxic effects and higher bowel-related quality of life in late follow-up.
Conflict of interest statement
Figures

References
-
- Kang MH, Yu YD, Shin HS, Oh JJ, Park DS. Difference in the rate of rectal complications following prostate brachytherapy based on the prostate-rectum distance and the prostate longitudinal length among early prostate cancer patients. Korean J Urol. 2015;56(9):637-643. doi: 10.4111/kju.2015.56.9.637 - DOI - PMC - PubMed
-
- Mariados N, Sylvester J, Shah D, et al. Hydrogel spacer prospective multicenter randomized controlled pivotal trial: dosimetric and clinical effects of perirectal spacer application in men undergoing prostate image guided intensity modulated radiation therapy. Int J Radiat Oncol Biol Phys. 2015;92(5):971-977. doi: 10.1016/j.ijrobp.2015.04.030 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
