

The predictive value of variables measurable in the ambulance and the development of the Predict Sepsis screening tools: a prospective cohort study
- PMID: 32586337
- PMCID: PMC7318751
- DOI: 10.1186/s13049-020-00745-6
The predictive value of variables measurable in the ambulance and the development of the Predict Sepsis screening tools: a prospective cohort study
Abstract
Background: Despite sepsis being a time critical condition with a high mortality, it is often not identified in a timely fashion. The aim of the current study was to create a screening tool based on bedside measurable variables predictive of sepsis among ambulance patients with infection according to clinical judgment by ambulance personnel.
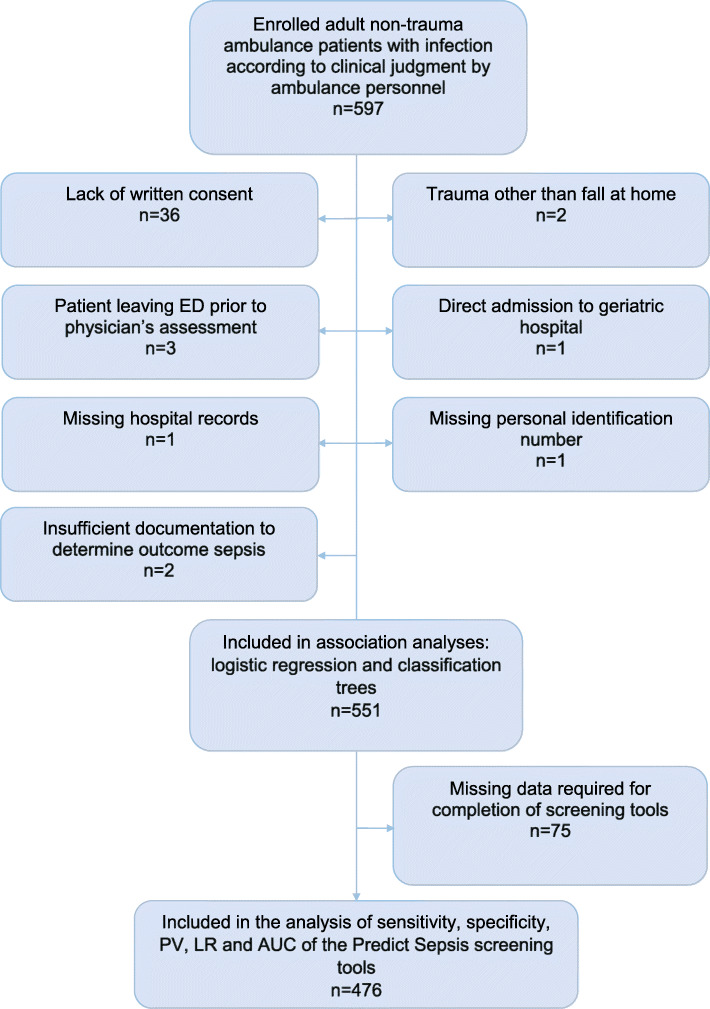
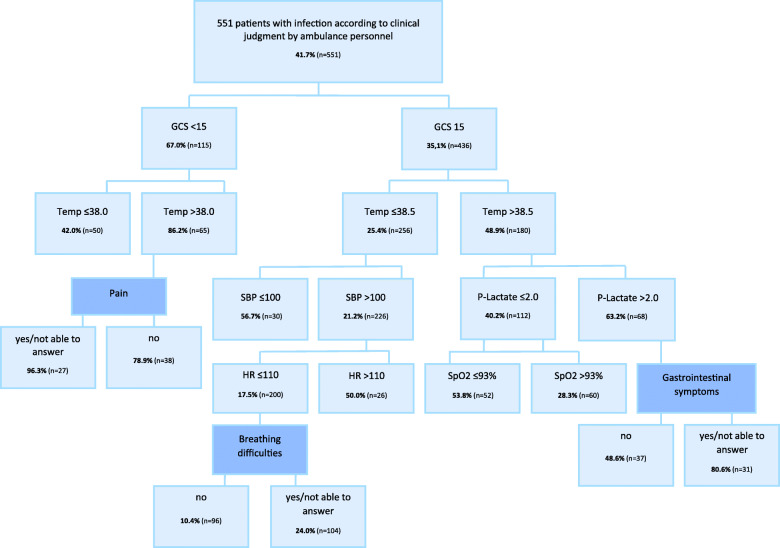
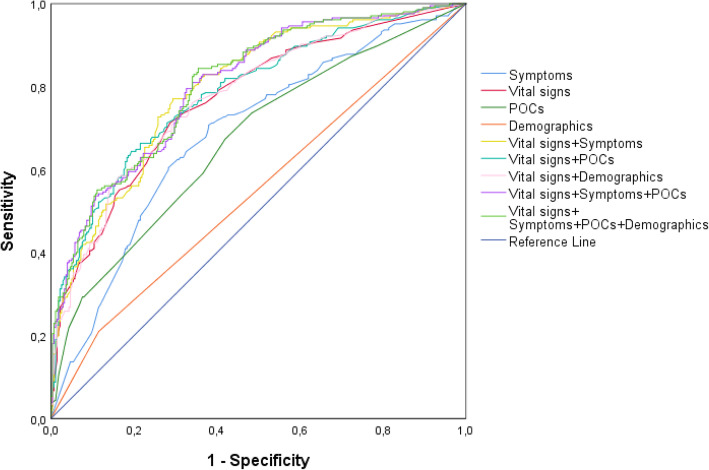
Methods: Prospective cohort study of 551 adult patients presenting with suspected infection, performed in the ambulance setting of Stockholm during 2017-2018. 18 variables were measured in the ambulance (8 keywords related to medical history, 6 vital signs, 4 point-of-care blood tests, in addition to age, gender, and comorbidity. Logistic regression, area under the curve (AUC) and classification trees were used to study the association with sepsis. The AUC, sensitivity, specificity, predictive values and likelihood ratios were used to evaluate the predictive ability of sepsis screening models.
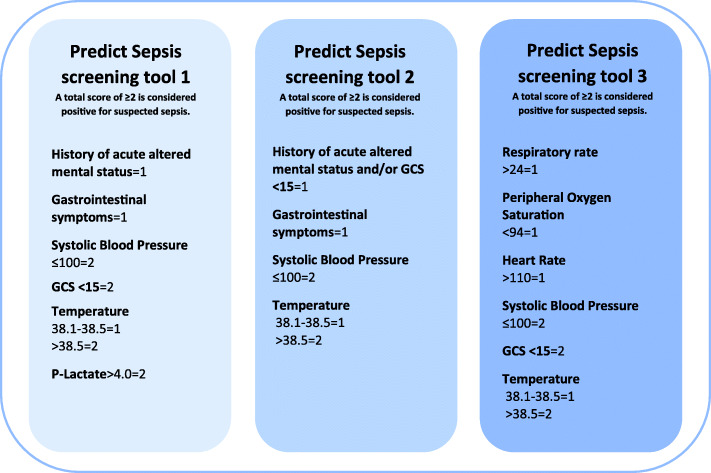
Results: The six variables with the strongest association with sepsis were: systolic blood pressure ≤ 100 mmHg, temperature > 38.5 °C, GCS < 15, lactate > 4 mmol/L, gastrointestinal symptoms, and a history of acute altered mental status. These were combined into the Predict Sepsis screening tool 1, with a sensitivity of 0.90, specificity 0.41, AUC 0.77; 95% confidence interval [CI] 0.73-0.81, PPV 0.52, and NPV 0.86. Combining a history of acute altered mental status with GCS < 15 and excluding lactate in the Predict Sepsis screening tool 2 did not noticeably affect the AUC. In addition, the AUCs of these models did not differ noticeably when compared to a model including vital signs alone, with novel calculated cut-offs; the Predict Sepsis screening tool 3.
Conclusions: Systolic blood pressure ≤ 100 mmHg, temperature > 38.5 °C, GCS < 15, lactate > 4 mmol/L, gastrointestinal symptoms, and a history of acute altered mental status demonstrated the strongest association with sepsis. We present three screening tools to predict sepsis with similar sensitivity. The results indicated no noticeable increase of predictive ability by including symptom-variables and blood tests to a sepsis screening tool in the current study population.
Trial registration: NCT03249597.
Keywords: Emergency care; Emergency medical services; Prehospital; Screening; Sepsis.
Conflict of interest statement
All authors declare that they have no conflicting interests. UW and LK are members of the Swedish national working group for sepsis and LK is chair of the Swedish national working group for emergency medicine.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
