

Electrocardiographic features of patients with COVID-19 pneumonia
- PMID: 32586646
- PMCID: PMC7305928
- DOI: 10.1016/j.ejim.2020.06.015
Electrocardiographic features of patients with COVID-19 pneumonia
Abstract
Background: . The electrocardiographic (ECG) changes which may occur during hospitalization for COVID-19 have not yet been comprehensively assessed.
Patients and methods: . We examined 50 patients admitted to hospital with proven COVID-19 pneumonia. At entry, all patients underwent a detailed clinical examination, 12-lead ECG, laboratory tests and arterial blood gas test. ECG was also recorded at discharge and in case of worsening clinical conditions.
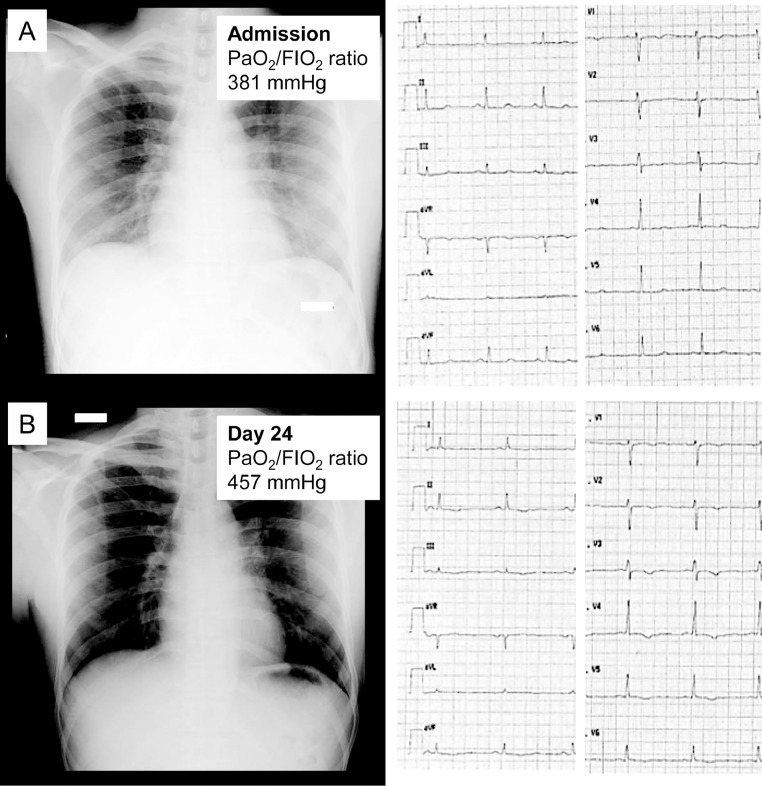
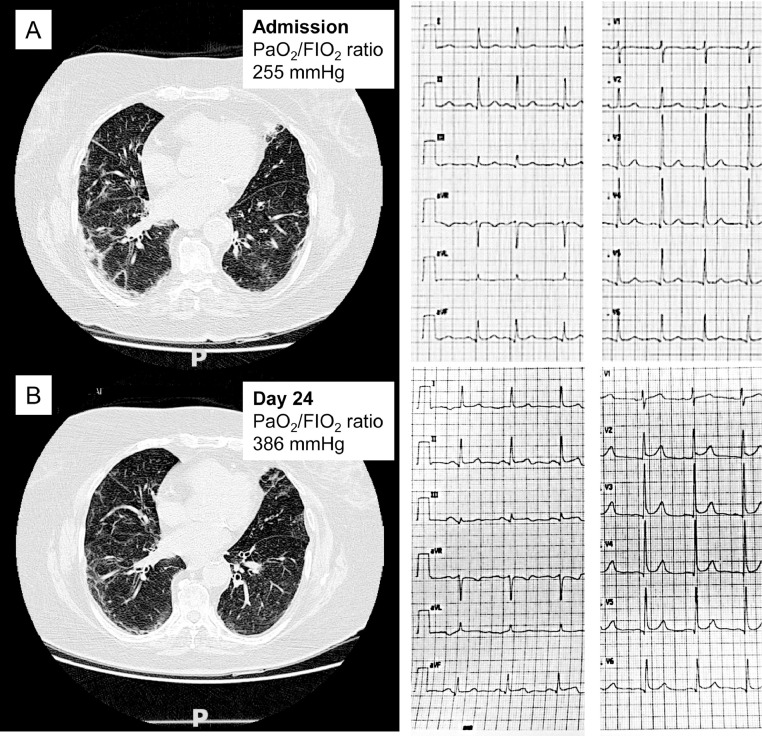
Results: . Mean age of patients was 64 years and 72% were men. At baseline, 30% of patients had ST-T abnormalities, and 33% had left ventricular hypertrophy. During hospitalization, 26% of patients developed new ECG abnormalities which included atrial fibrillation, ST-T changes, tachy-brady syndrome, and changes consistent with acute pericarditis. One patient was transferred to intensive care unit for massive pulmonary embolism with right bundle branch block, and another for non-ST segment elevation myocardial infarction. Patients free of ECG changes during hospitalization were more likely to be treated with antiretrovirals (68% vs 15%, p = 0.001) and hydroxychloroquine (89% vs 62%, p = 0.026) versus those who developed ECG abnormalities after admission. Most measurable ECG features at discharge did not show significant changes from baseline (all p>0.05) except for a slightly decrease in Cornell voltages (13±6 vs 11±5 mm; p = 0.0001) and a modest increase in the PR interval. The majority (54%) of patients with ECG abnormalities had 2 prior consecutive negative nasopharyngeal swabs. ECG abnormalities were first detected after an average of about 30 days from symptoms' onset (range 12-51 days).
Conclusions: . ECG abnormalities during hospitalization for COVID-19 pneumonia reflect a wide spectrum of cardiovascular complications, exhibit a late onset, do not progress in parallel with pulmonary abnormalities and may occur after negative nasopharyngeal swabs.
Keywords: COVID-19; Electrocardiography; Heart; Prognosis; SARS-CoV-2.
Copyright © 2020 European Federation of Internal Medicine. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
