

Treatment options in type-2 low asthma
- PMID: 32586877
- PMCID: PMC7116624
- DOI: 10.1183/13993003.00528-2020
Treatment options in type-2 low asthma
Abstract
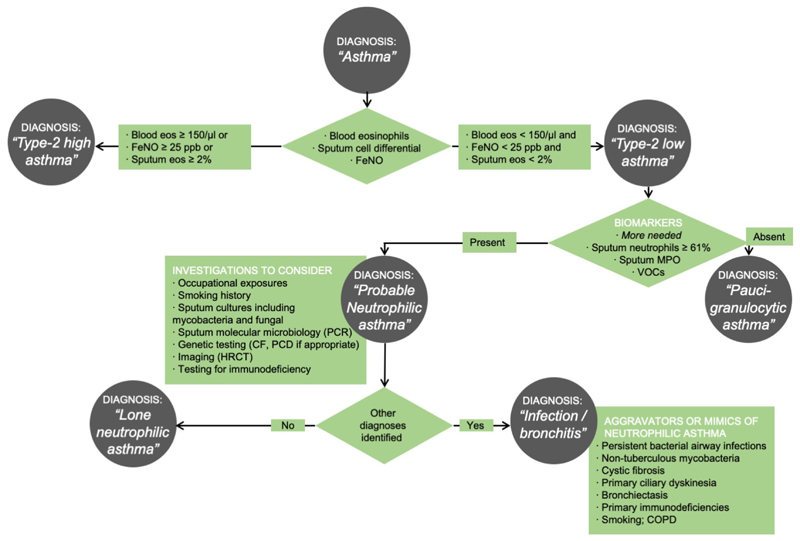
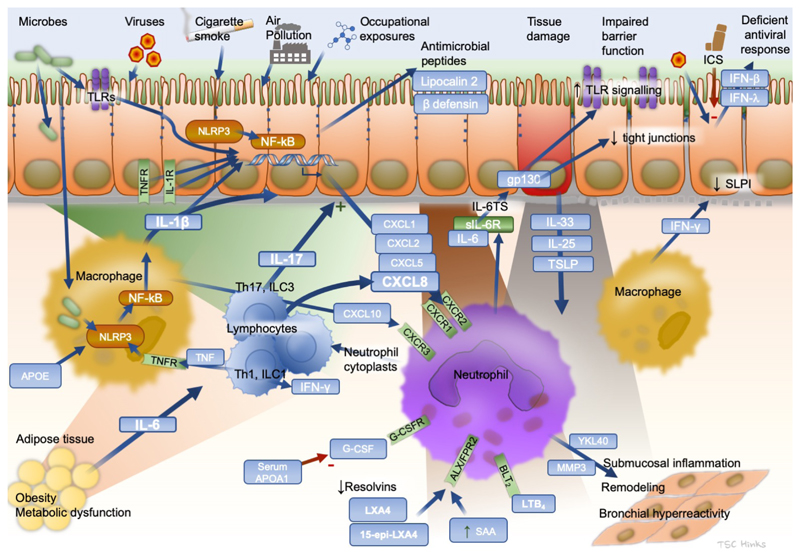
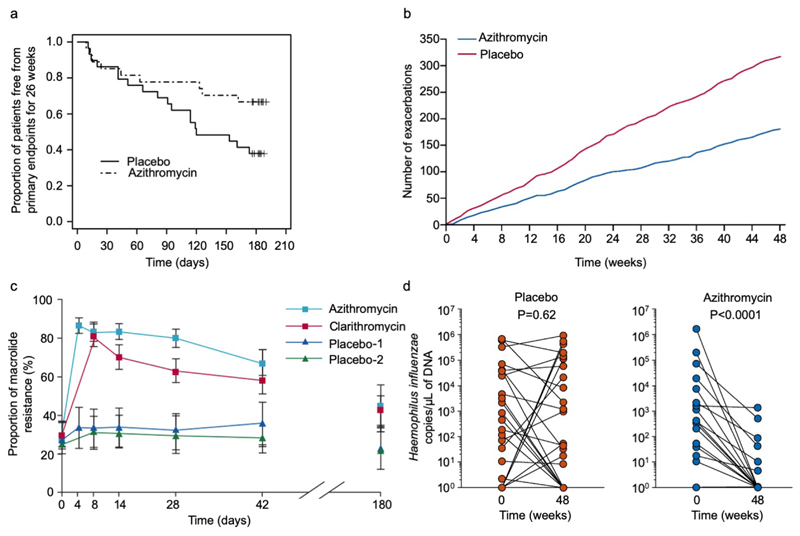
Monoclonal antibodies targeting IgE or the type-2 cytokines interleukin (IL)-4, IL-5 and IL-13 are proving highly effective in reducing exacerbations and symptoms in people with severe allergic and eosinophilic asthma, respectively. However, these therapies are not appropriate for 30-50% of patients in severe asthma clinics who present with non-allergic, non-eosinophilic, "type-2 low" asthma. These patients constitute an important and common clinical asthma phenotype, driven by distinct, yet poorly understood pathobiological mechanisms. In this review we describe the heterogeneity and clinical characteristics of type-2 low asthma and summarise current knowledge on the underlying pathobiological mechanisms, which includes neutrophilic airway inflammation often associated with smoking, obesity and occupational exposures and may be driven by persistent bacterial infections and by activation of a recently described IL-6 pathway. We review the evidence base underlying existing treatment options for specific treatable traits that can be identified and addressed. We focus particularly on severe asthma as opposed to difficult-to-treat asthma, on emerging data on the identification of airway bacterial infection, on the increasing evidence base for the use of long-term low-dose macrolides, a critical appraisal of bronchial thermoplasty, and evidence for the use of biologics in type-2 low disease. Finally, we review ongoing research into other pathways including tumour necrosis factor, IL-17, resolvins, apolipoproteins, type I interferons, IL-6 and mast cells. We suggest that type-2 low disease frequently presents opportunities for identification and treatment of tractable clinical problems; it is currently a rapidly evolving field with potential for the development of novel targeted therapeutics.
The content of this work is not subject to copyright. Design and branding are copyright ©ERS 2021.
Conflict of interest statement
Conflict of interest: T.S.C. Hinks reports grants from The Wellcome Trust (Wellcome Trust Fellowships 088365/z/09/z, 104553/Z/14/Z, 211050/Z/18/Z) and the Guardians of the Beit Fellowship (Wellcome-Beit Fellowship 211050/Z/18/A), during the conduct of the study; personal fees for lectures from AstraZeneca and TEVA, personal fees for education presentations from Peer Voice, outside the submitted work. Conflict of interest: S.J. Levine has nothing to disclose. Conflict of interest: G.G. Brusselle reports personal fees for advisory board work and lectures from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis and Teva, personal fees for advisory board work from Sanofi, outside the submitted work.
Figures
References
-
- Lambrecht BN, Hammad H, Fahy JV. The Cytokines of Asthma. Immunity. 2019;50(4):975–991. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical