

Leukoencephalopathy Associated with Severe COVID-19 Infection: Sequela of Hypoxemia?
- PMID: 32586959
- PMCID: PMC7583106
- DOI: 10.3174/ajnr.A6671
Leukoencephalopathy Associated with Severe COVID-19 Infection: Sequela of Hypoxemia?
Abstract
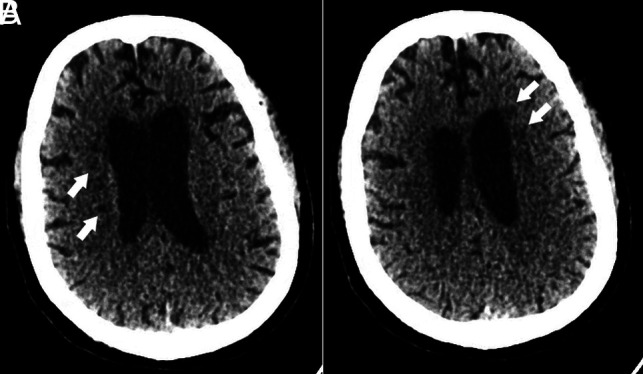
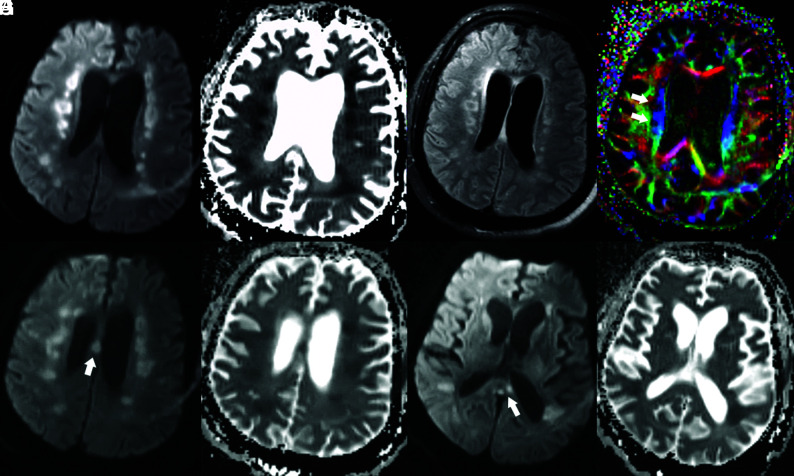
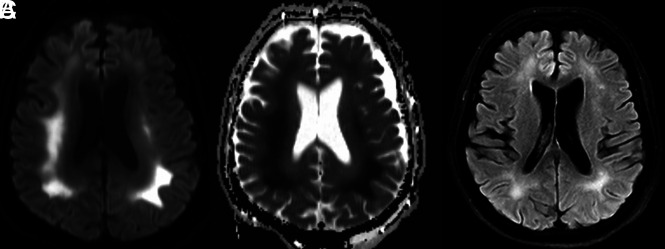
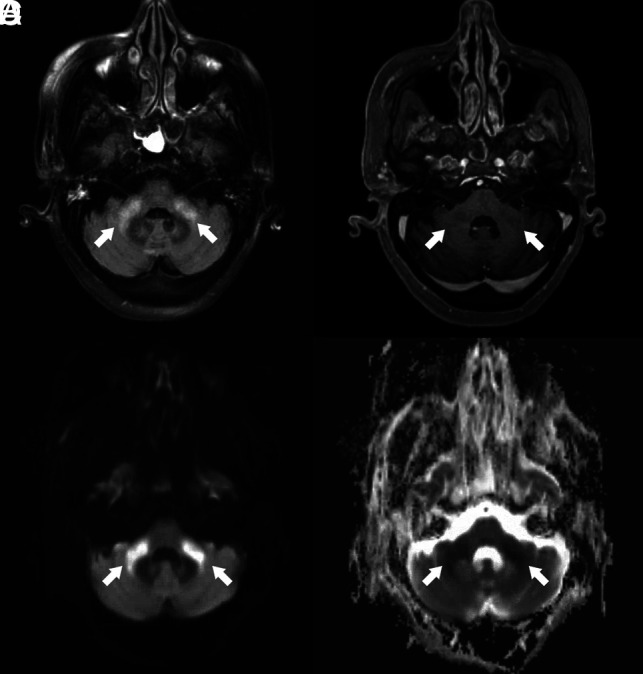
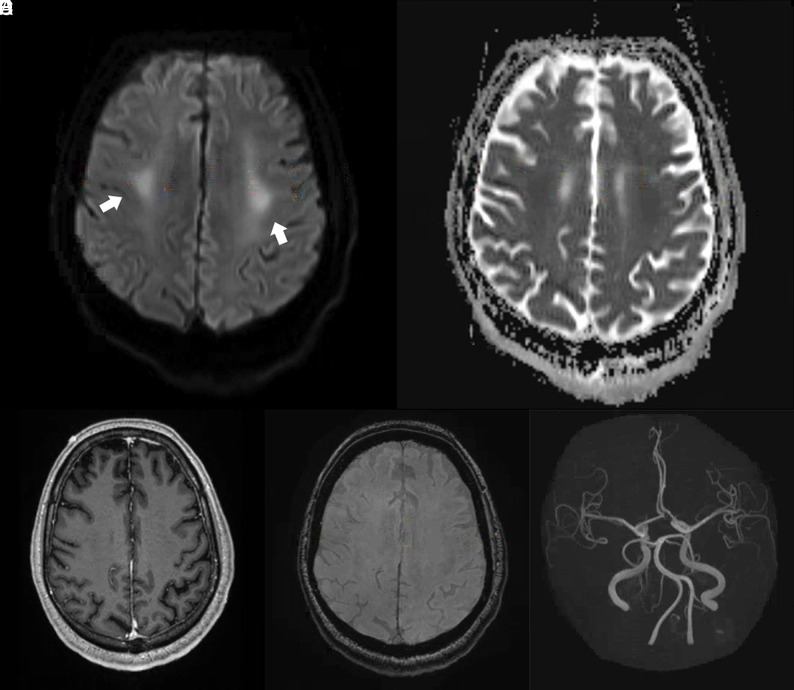
There is increasing evidence to suggest that complications of coronavirus disease 2019 (COVID-19) infection are not only limited to the pulmonary system but can also involve the central nervous system. Here, we report 6 critically ill patients with COVID-19 infection and neuroimaging findings of leukoencephalopathy. While these findings are nonspecific, we postulate that they may be a delayed response to the profound hypoxemia the patients experienced due to the infection. No abnormal enhancement, hemorrhage, or perfusion abnormalities were noted on MR imaging. In addition, Severe Acute Respiratory Syndrome coronavirus 2 was not detected in the CSF collected from the 2 patients who underwent lumbar puncture. Recognition of COVID-19-related leukoencephalopathy is important for appropriate clinical management, disposition, and prognosis.
© 2020 by American Journal of Neuroradiology.
Figures
Comment in
-
Level of Evidence during the COVID-19 Pandemic: Making the Case for Case Series and Case Reports.AJNR Am J Neuroradiol. 2020 Sep;41(9):1646. doi: 10.3174/ajnr.A6676. Epub 2020 Jul 2. AJNR Am J Neuroradiol. 2020. PMID: 32616587 Free PMC article. No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources