

Variable Refocusing Flip Angle Single-Shot Imaging for Sedation-Free Fast Brain MRI
- PMID: 32586967
- PMCID: PMC7357630
- DOI: 10.3174/ajnr.A6616
Variable Refocusing Flip Angle Single-Shot Imaging for Sedation-Free Fast Brain MRI
Abstract
Background and purpose: Conventional single-shot FSE commonly used for fast MRI may be suboptimal for brain evaluation due to poor image contrast, SNR, or image blurring. We investigated the clinical performance of variable refocusing flip angle single-shot FSE, a variation of single-shot FSE with lower radiofrequency energy deposition and potentially faster acquisition time, as an alternative approach to fast brain MR imaging.
Materials and methods: We retrospectively compared half-Fourier single-shot FSE with half- and full-Fourier variable refocusing flip angle single-shot FSE in 30 children. Three readers reviewed images for motion artifacts, image sharpness at the brain-fluid interface, and image sharpness/tissue contrast at gray-white differentiation on a modified 5-point Likert scale. Two readers also evaluated full-Fourier variable refocusing flip angle single-shot FSE against T2-FSE for brain lesion detectability in 38 children.
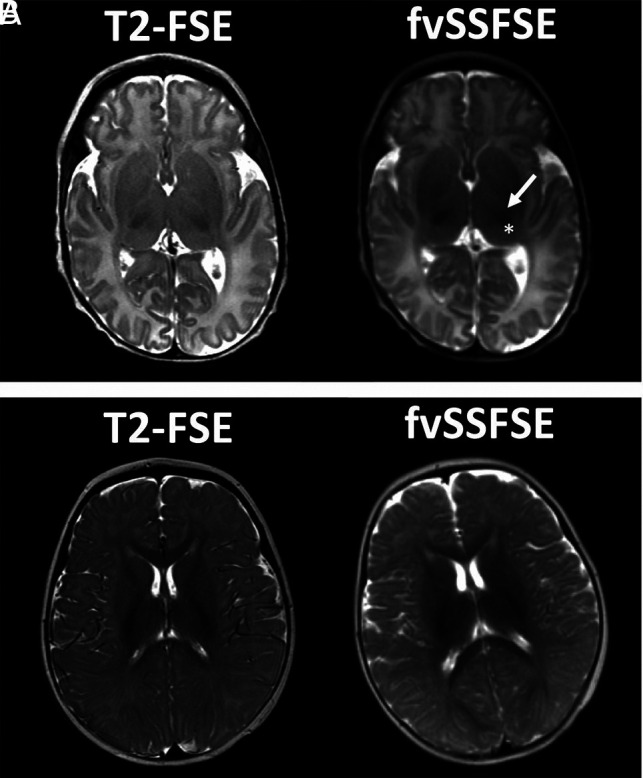
Results: Variable refocusing flip angle single-shot FSE sequences showed more motion artifacts (P < .001). Variable refocusing flip angle single-shot FSE sequences scored higher regarding image sharpness at brain-fluid interfaces (P < .001) and gray-white differentiation (P < .001). Acquisition times for half- and full-Fourier variable refocusing flip angle single-shot FSE were faster than for single-shot FSE (P < .001) with a 53% and 47% reduction, respectively. Intermodality agreement between full-Fourier variable refocusing flip angle single-shot FSE and T2-FSE findings was near-perfect (κ = 0.90, κ = 0.95), with an 8% discordance rate for ground truth lesion detection.
Conclusions: Variable refocusing flip angle single-shot FSE achieved 2× faster scan times than single-shot FSE with improved image sharpness at brain-fluid interfaces and gray-white differentiation. Such improvements are likely attributed to a combination of improved contrast, spatial resolution, SNR, and reduced T2-decay associated with blurring. While variable refocusing flip angle single-shot FSE may be a useful alternative to single-shot FSE and, potentially, T2-FSE when faster scan times are desired, motion artifacts were more common in variable refocusing flip angle single-shot FSE, and, thus, they remain an important consideration before clinical implementation.
© 2020 by American Journal of Neuroradiology.
Figures





References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical