

Role of adjuvant carotid ultrasound in women undergoing stress echocardiography for the assessment of suspected coronary artery disease
- PMID: 32587105
- PMCID: PMC7319702
- DOI: 10.1136/openhrt-2019-001188
Role of adjuvant carotid ultrasound in women undergoing stress echocardiography for the assessment of suspected coronary artery disease
Abstract
Objective: Due to the low prevalence of obstructive coronary artery disease (CAD) in women, stress testing has a relatively low predictive value for this. Additionally, conventional cardiovascular risk scores underestimate risk in women. This study sought to evaluate the role of atherosclerosis assessment using carotid ultrasound (CU) in women attending for stress echocardiography (SE).
Methods: This was a prospective study in which consecutive women with recent-onset suspected angina, who were referred for clinically indicated SE, underwent CU.
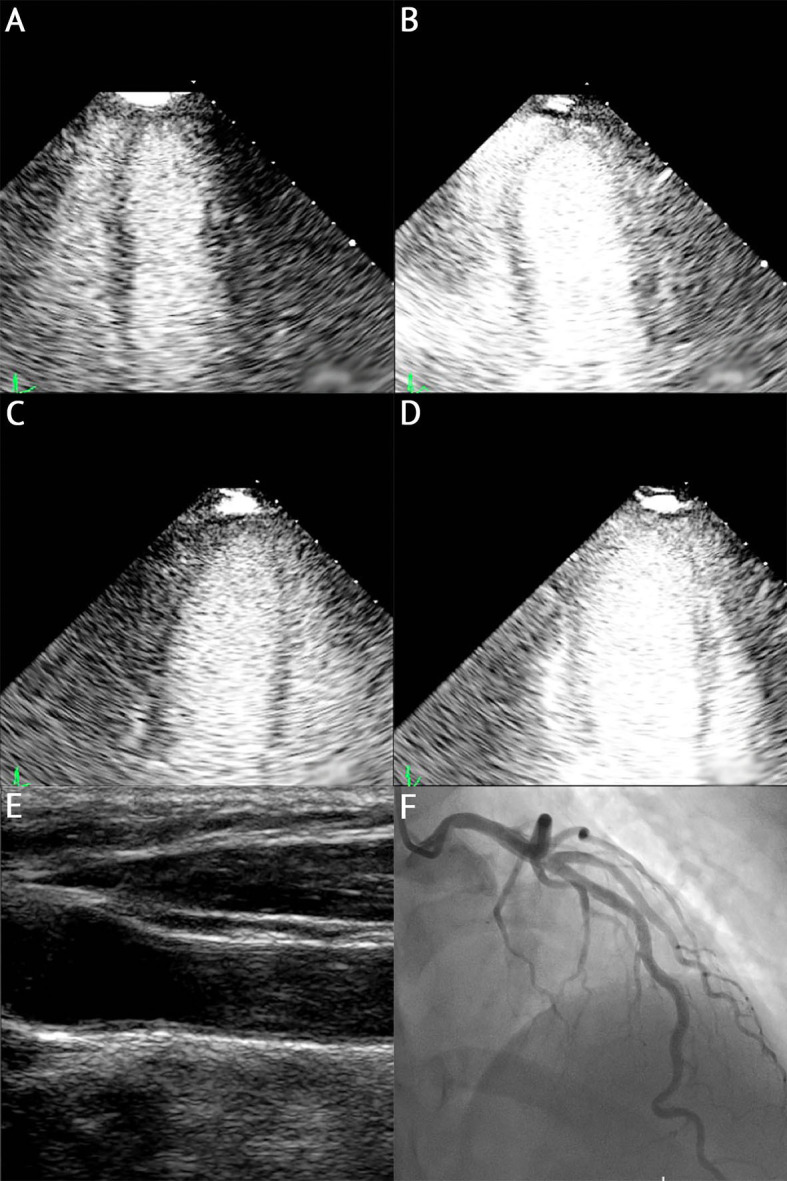
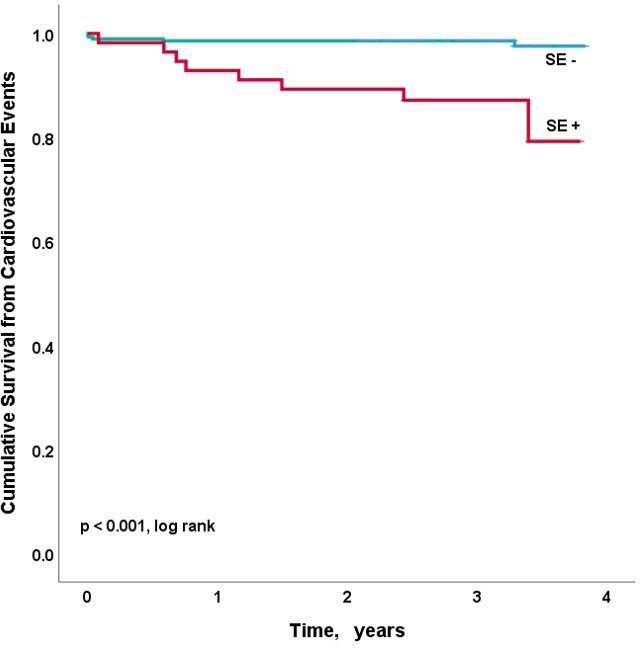
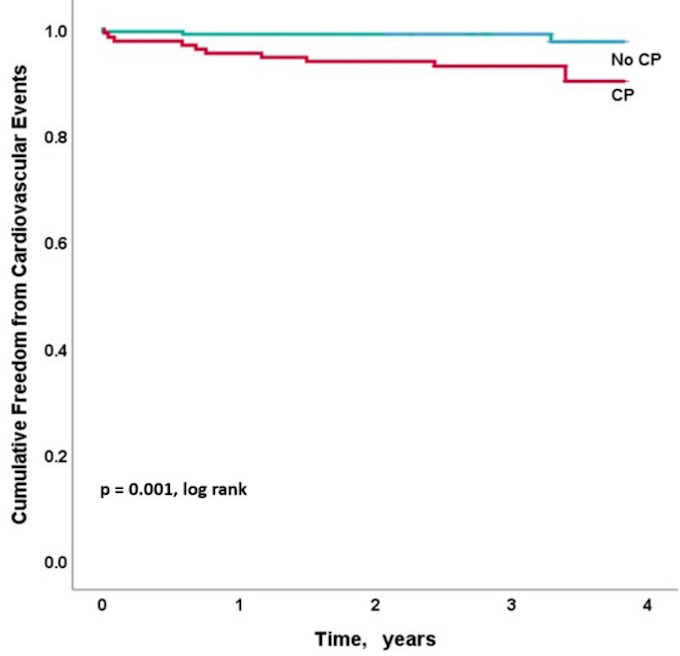
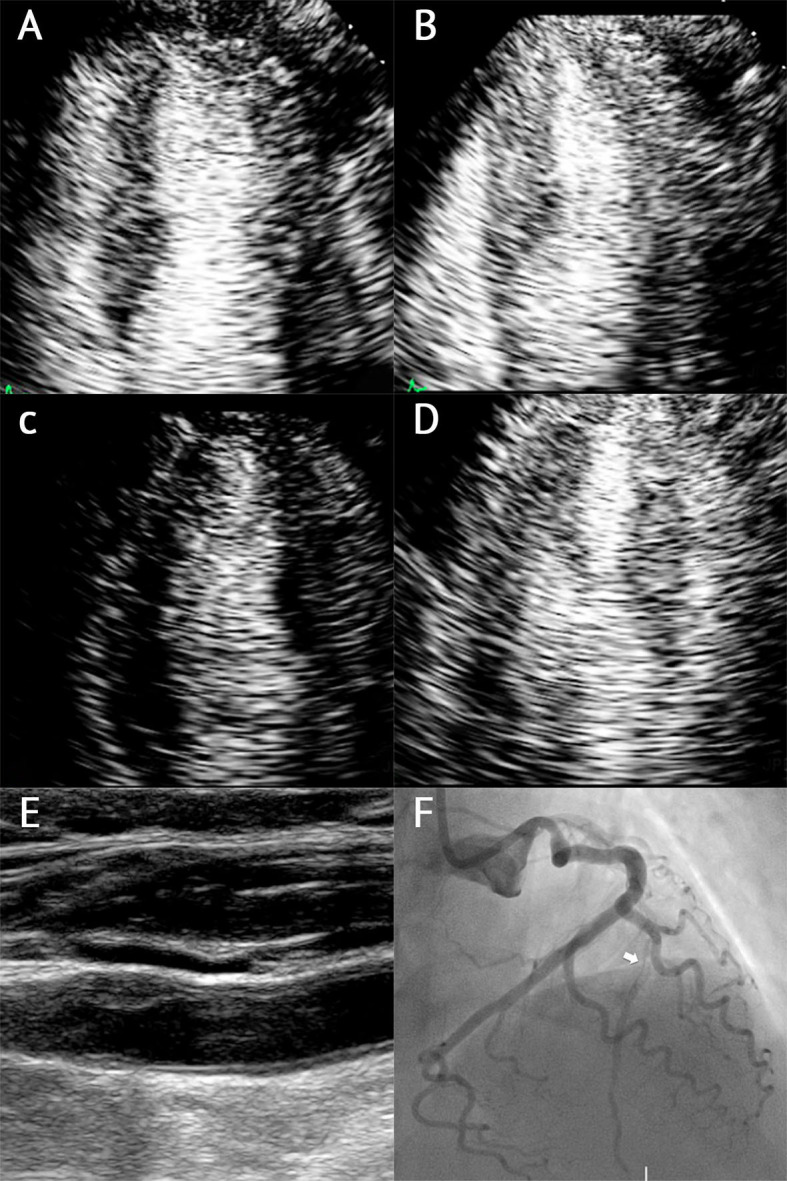
Results: 415 women (mean age 61±10 years, 29% diabetes mellitus, mean body mass index 28) attending for SE underwent CU. 47 women (11%) had inducible wall motion abnormalities, and carotid disease (CD) was present in 46% (carotid plaque in 41%, carotid intima-media thickness >75th percentile in 15%). Women with CD were older (65 vs 58 years, p<0.001), and more likely to have diabetes (41% vs 21%, p=0.001), hypertension (67% vs 36%, p<0.01) and a higher pretest probability of CAD (59% vs 41%, p<0.001). 40% of women classified as low Framingham risk were found to have evidence of CD.The positive predictive value of SE for flow-limiting CAD was 51%, but with the presence of carotid plaque, this was 71% (p<0.01). Carotid plaque (p=0.004) and ischaemia (p=0.01) were the only independent predictors of >70% angiographic stenosis. In women with ischaemia on SE and no carotid plaque, the negative predictive value for flow-limiting disease was 88%.During a follow-up of 1058±234 days, there were 15 events (defined as all-cause mortality, non-fatal myocardial infarction, heart failure admissions and late coronary revascularisation). Age (HR 1.07 (1.00-1.15), p=0.04), carotid plaque burden (HR 1.65 (1.36-2.00), p<0.001) and ischaemic burden (HR 1.41 (1.18-1.68), p<0.001) were associated with outcome. There was a stepwise increase in events/year from 0.3% when there were no ischaemia and atherosclerosis, 1.1% when there was atherosclerosis and no ischaemia, 2.2% when there was ischaemia and no atherosclerosis and 10% when there were both ischaemia and atherosclerosis (p<0.001).
Conclusion: CU significantly improves the accuracy of SE alone for identifying flow-limiting disease on coronary angiography, and improves risk stratification in women attending for SE, as well identifying a subset of women who may benefit from primary preventative measures.
Keywords: atherosclerosis; carotid artery disease; stress.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: RS has received speaker fees from Bracco (Italy), Phillips (Netherlands) and Lantheus Medical Imaging.
Figures
Similar articles
-
Sex-based impact of carotid plaque in patients with chest pain undergoing stress echocardiography.Heart. 2020 Dec;106(23):1819-1823. doi: 10.1136/heartjnl-2019-316507. Epub 2020 May 22. Heart. 2020. PMID: 32444505
-
Incremental Prognostic Value of Stress Echocardiography With Carotid Ultrasound for Suspected CAD.JACC Cardiovasc Imaging. 2018 Feb;11(2 Pt 1):173-180. doi: 10.1016/j.jcmg.2016.12.020. Epub 2017 Apr 12. JACC Cardiovasc Imaging. 2018. PMID: 28412430
-
Role of simultaneous carotid ultrasound in patients undergoing stress echocardiography for assessment of chest pain with no previous history of coronary artery disease.Am Heart J. 2014 Aug;168(2):229-36. doi: 10.1016/j.ahj.2014.04.016. Epub 2014 May 15. Am Heart J. 2014. PMID: 25066563
-
Stress Echocardiography in Stable Coronary Artery Disease.Curr Cardiol Rep. 2017 Oct 18;19(12):121. doi: 10.1007/s11886-017-0935-x. Curr Cardiol Rep. 2017. PMID: 29046974 Review.
-
Carotid ultrasound assessment of patients with coronary artery disease: a useful index for risk stratification.Vasc Health Risk Manag. 2005;1(2):131-6. doi: 10.2147/vhrm.1.2.131.64077. Vasc Health Risk Manag. 2005. PMID: 17315399 Free PMC article. Review.
Cited by
-
ICEBERG-3: carotid plaque score combined with the stress echo improves 5-year major adverse cardiovascular events risk prediction.Eur Heart J Open. 2025 Jun 2;5(3):oeaf065. doi: 10.1093/ehjopen/oeaf065. eCollection 2025 May. Eur Heart J Open. 2025. PMID: 40520409 Free PMC article.
-
Determination of the Level of Cardiovascular Risk in 172,282 Spanish Working Women.Diagnostics (Basel). 2023 Aug 23;13(17):2734. doi: 10.3390/diagnostics13172734. Diagnostics (Basel). 2023. PMID: 37685272 Free PMC article.
-
Multimodality imaging: Bird's eye view from the European Society of Cardiology Congress 2019 Paris, August 31st-September 4th, 2019.J Nucl Cardiol. 2020 Feb;27(1):53-61. doi: 10.1007/s12350-019-01958-8. Epub 2019 Nov 18. J Nucl Cardiol. 2020. PMID: 31741328 Free PMC article. Review.
References
-
- WHO Global health Observatory (GHO) data. Available: https://www.who.int/gho/women_and_health/en/
-
- Shaw LJ, Merz CNB, Pepine CJ, et al. . The economic burden of angina in women with suspected ischemic heart disease: results from the National Institutes of Health--National Heart, Lung, and Blood Institute--sponsored Women's Ischemia Syndrome Evaluation. Circulation 2006;114:894–904. 10.1161/CIRCULATIONAHA.105.609990 - DOI - PubMed
-
- Mieres JH, Shaw LJ, Arai A, Gulati M, Bairey Merz N, et al. . Role of noninvasive testing in the clinical evaluation of women with suspected coronary artery disease: consensus statement from the cardiac imaging Committee, Council on clinical cardiology, and the cardiovascular imaging and intervention Committee, Council on cardiovascular radiology and intervention, American heart association. Circulation 2005;111:350–79. 10.1161/01.CIR.0000155233.67287.60 - DOI - PubMed
-
- Shaw esleeJ, Gibbons RJ, McCallister B, et al. . Gender differences in extent and severity of coronary disease in the ACC national cardiovascular disease registry. J Am Coll Cardiol 2002;39:321 10.1016/S0735-1097(02)81444-9 - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous