

Bevacizumab promotes active biological behaviors of human umbilical vein endothelial cells by activating TGFβ1 pathways via off-VEGF signaling
- PMID: 32587778
- PMCID: PMC7309466
- DOI: 10.20892/j.issn.2095-3941.2019.0215
Bevacizumab promotes active biological behaviors of human umbilical vein endothelial cells by activating TGFβ1 pathways via off-VEGF signaling
Abstract
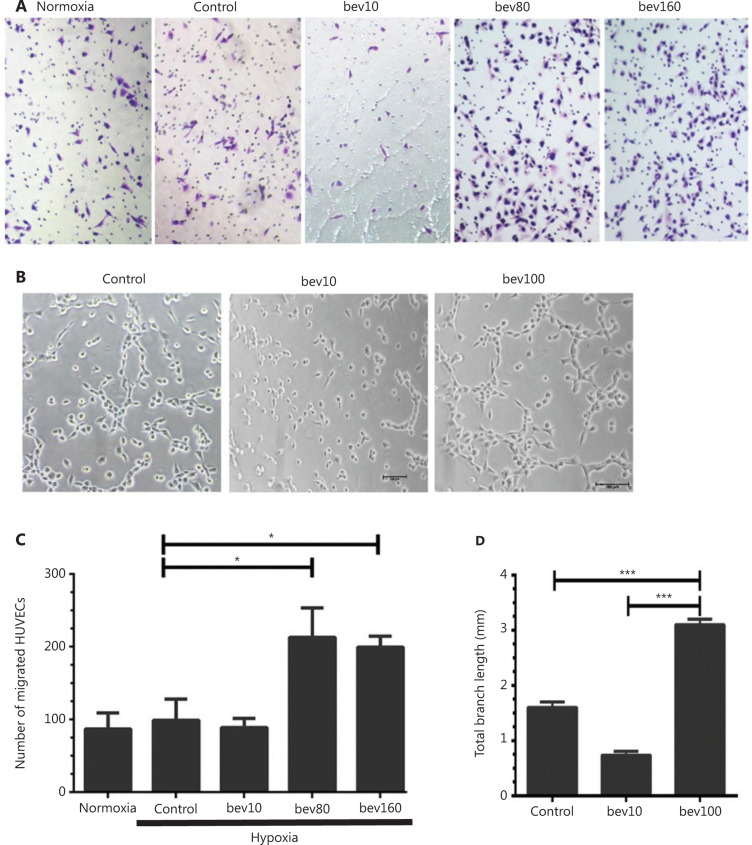
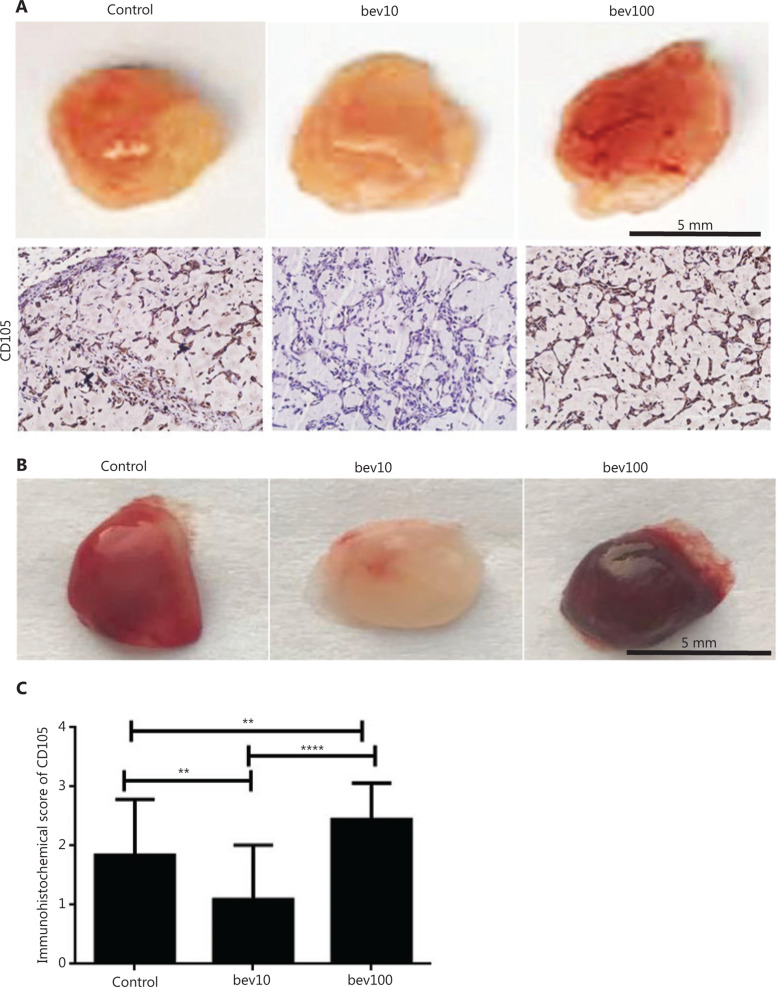
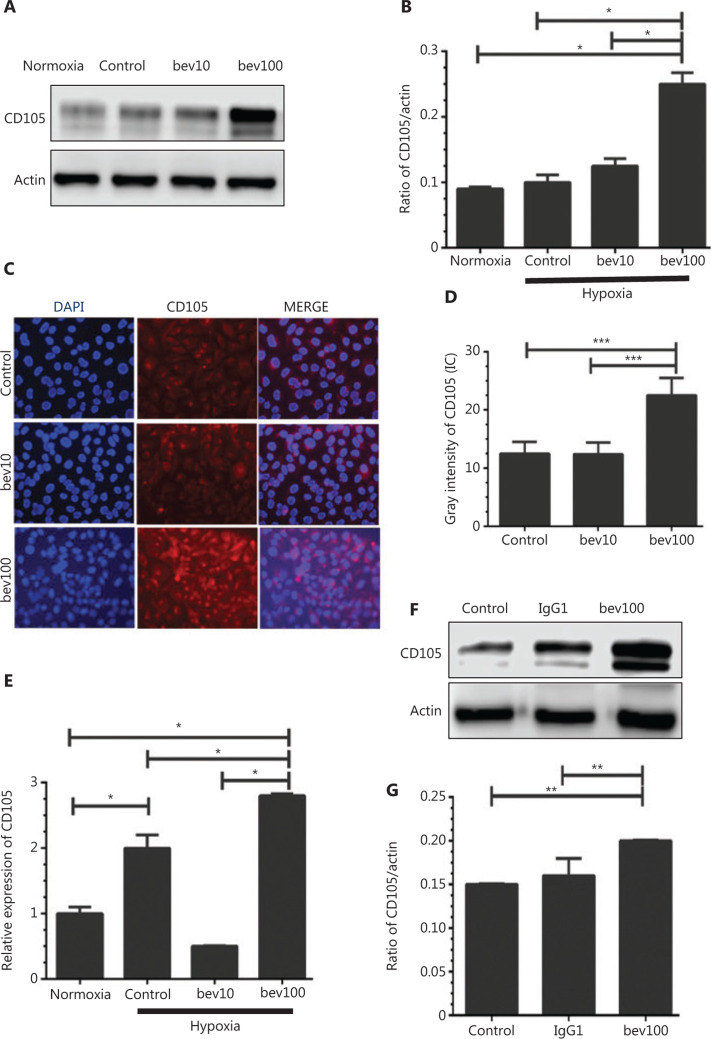
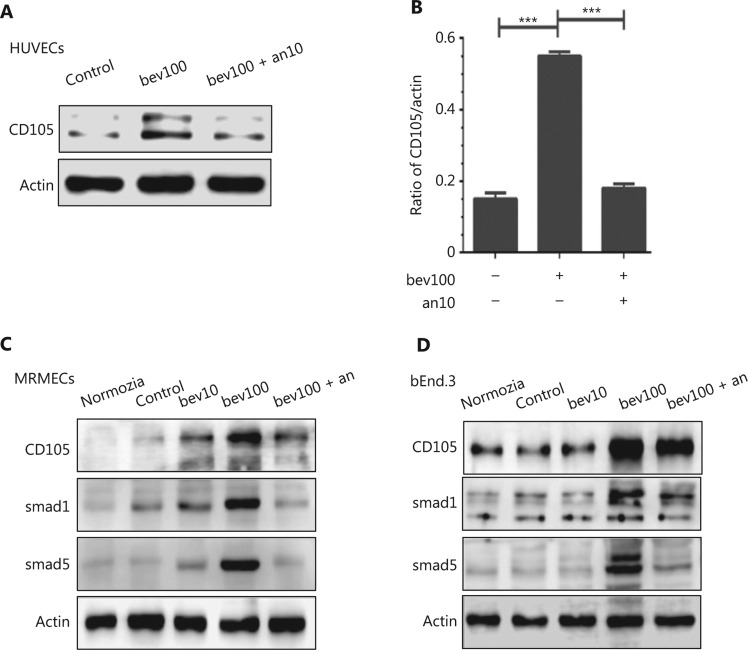
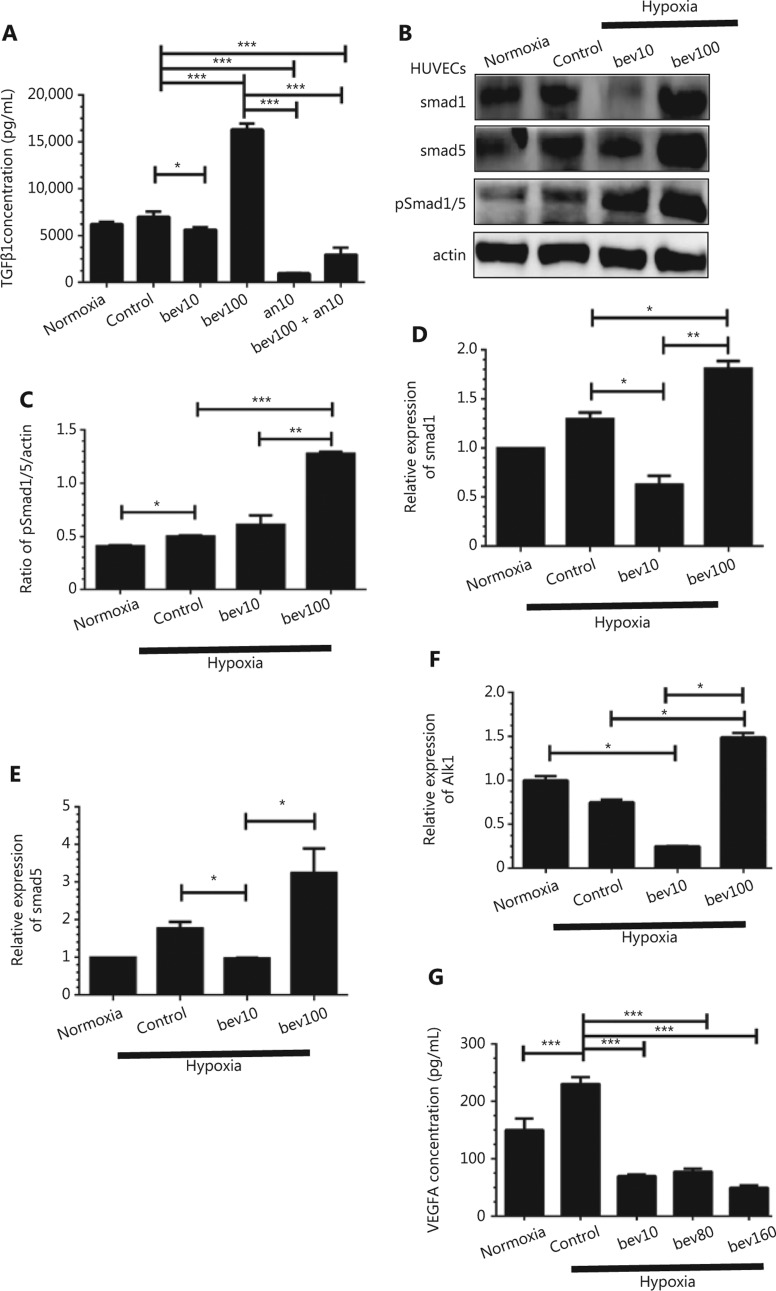
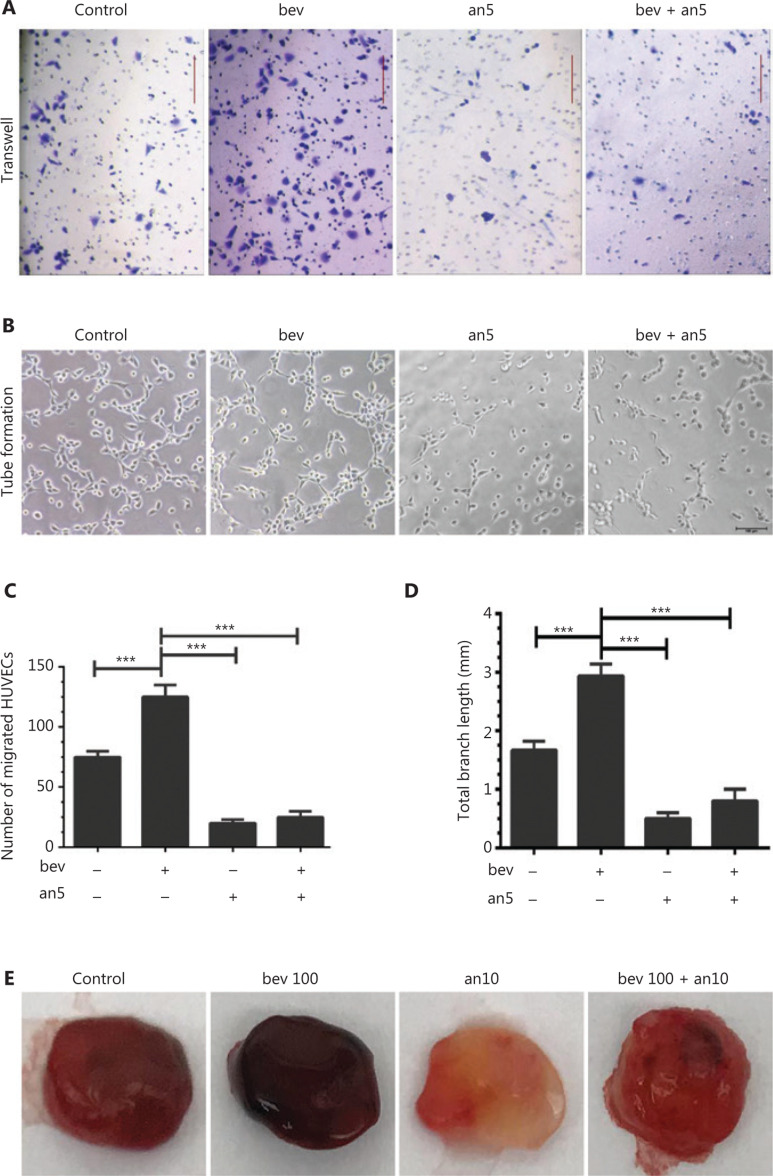
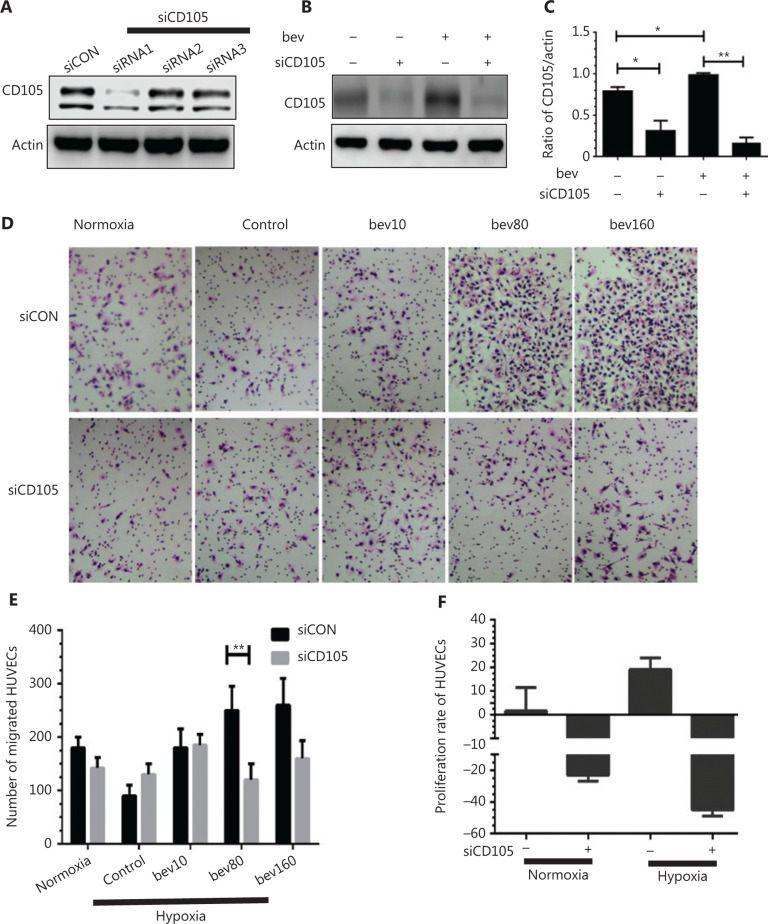
Objective: Bevacizumab is a recombinant humanized monoclonal antibody that blocks vascular endothelial growth factor (VEGF) with clear clinical benefits. However, overall survival of some cancer types remains low owing to resistance to bevacizumab therapy. While resistance is commonly ascribed to tumor cell invasion induced by hypoxia-inducible factor (HIF), less attention has been paid to the potential involvement of endothelial cells (ECs) in vasculature activated by anti-angiogenic drugs. Methods: Human umbilical vein ECs (HUVECs), bEnd.3 cells, and mouse retinal microvascular ECs (MRMECs) were treated with bevacizumab under conditions of hypoxia and effects on biological behaviors, such as migration and tube formation, examined. Regulatory effects on TGFβ1 and CD105 (endoglin) were established via determination of protein and mRNA levels. We further investigated whether the effects of bevacizumab could be reversed using the receptor tyrosine kinase inhibitor anlotinib. Results: Bevacizumab upregulated TGFβ1 as well as CD105, a component of the TGFβ receptor complex and an angiogenesis promoter. Elevated CD105 induced activation of Smad1/5, the inflammatory pathway and endothelial-mesenchymal transition. The migration ability of HUVECs was enhanced by bevacizumab under hypoxia. Upregulation of CD105 was abrogated by anlotinib, which targets multiple receptor tyrosine kinases including VEGFR2/3, FGFR1-4, PDGFRα/β, C-Kit, and RET. Conclusions: Bevacizumab promotes migration and tube formation of HUVECs via activation of the TGFβ1 pathway and upregulation of CD105 expression. Anlotinib reverses the effects of bevacizumab by inhibiting the above signals.
Keywords: CD105; HUVEC; TGFβ; anlotinib; bevacizumab.
Copyright: © 2020, Cancer Biology & Medicine.
Conflict of interest statement
*These authors contributed equally to this work.
Figures
References
-
- Chu BF, Otterson GA. Incorporation of antiangiogenic therapy into the non-small-cell lung cancer paradigm. Clin Lung Cancer. 2016;17:493–506. - PubMed
-
- Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J, Heim W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350:2335–42. - PubMed
-
- Reck M, von Pawel J, Zatloukal P, Ramlau R, Gorbounova V, Hirsh V, et al. Overall survival with cisplatin-gemcitabine and bevacizumab or placebo as first-line therapy for nonsquamous non-small-cell lung cancer: results from a randomised phase III trial (AVAiL). Ann Oncol. 2010;21:1804–9. - PMC - PubMed
-
- Robert NJ, Dieras V, Glaspy J, Brufsky AM, Bondarenko I, Lipatov ON, et al. RIBBON-1: randomized, double-blind, placebo-controlled, phase III trial of chemotherapy with or without bevacizumab for first-line treatment of human epidermal growth factor receptor 2-negative, locally recurrent or metastatic breast cancer. J Clin Oncol. 2011;29:1252–60. - PubMed
-
- Saltz LB, Clarke S, Diaz-Rubio E, Scheithauer W, Figer A, Wong R, et al. Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: a randomized phase III study. J Clin Oncol. 2008;26:2013–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous