

Defining benchmarks for tolerable risk thresholds in cancer screening: Impact of HPV vaccination on the future of cervical cancer screening
- PMID: 32588426
- PMCID: PMC7689748
- DOI: 10.1002/ijc.33178
Defining benchmarks for tolerable risk thresholds in cancer screening: Impact of HPV vaccination on the future of cervical cancer screening
Abstract
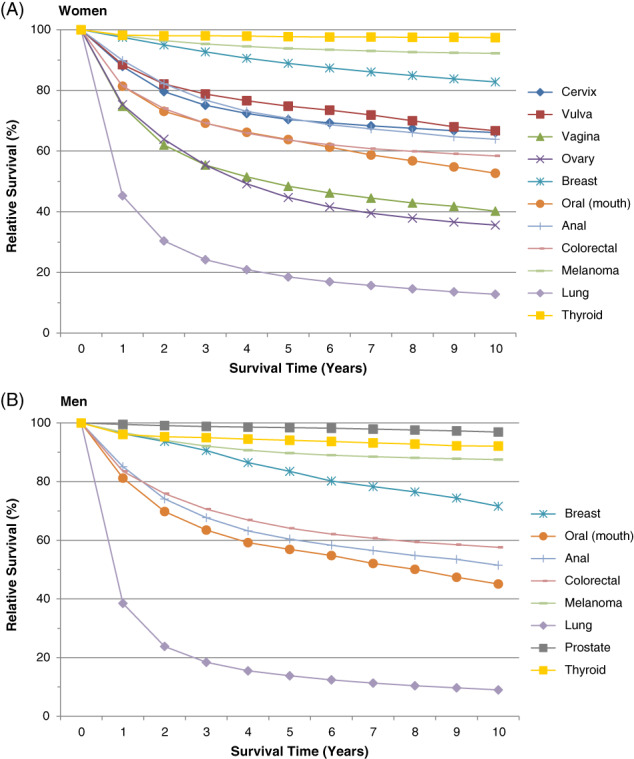
The performance of cervical cancer screening will decline as a function of lower disease prevalence-a consequence of successful human papillomavirus (HPV) vaccination. Replacement of cytology with molecular HPV testing as the primary screening test and adoption of risk-based screening, with less intense screening of vaccinated individuals and initiated at older ages is expected to improve efficiency. However, policy officials may decide to further reduce or eliminate screening as the ratio of benefits to harms continues to decline. To evaluate the level of risk currently tolerated for different cancers in the United States (ie, for which clinical guidelines do not recommend secondary prevention though effective screening methods exist), we used US cancer registry data to compare incidence (2008-2012) and survival (1988-2011) associated with different cancers for which organized screening is recommended and not recommended. The most common cancer at ages 70 to 74 years (ie, age group with highest cancer incidence and reasonable life expectancy to consider screening in the US) satisfying Wilson and Jungner's classic screening criteria was vulvar cancer (incidence = 9/100 000 females). In comparison, the incidence of cervical cancer among females 65 years of age (the upper recommended age limit for screening) was 13 cases per 100 000 females (low as a reflection of effective screening), whereas 10-year survival was 66% (similar to vulvar cancer at 67%). Our approach of defining tolerable risk in cancer screening could help guide future decisions to modify cervical screening programs.
Keywords: HPV vaccination; cervical cancer; screening; tolerable risk.
© 2020 The Authors. International Journal of Cancer published by John Wiley & Sons Ltd on behalf of Union for International Cancer Control.
Conflict of interest statement
J. E. T. is an employee of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA but completed all work associated with this manuscript while employed at the National Cancer Institute. E. L. F. does not have a conflict of interest with the content of this manuscript but has occasionally served as a consultant to Merck and GSK on HPV vaccines, and to Roche and BD on HPV diagnostics. His institution received unrestricted grants from Merck and Roche. S. D. I. declared no potential conflicts of interest.
Figures

References
-
- Li N, Franceschi S, Howell‐Jones R, Snijders PJ, Clifford GM. Human papillomavirus type distribution in 30,848 invasive cervical cancers worldwide: variation by geographical region, histological type and year of publication. Int J Cancer. 2011;128:927‐935. - PubMed
-
- Franco EL, Cuzick J, Hildesheim A, de Sanjose S. Chapter 20: issues in planning cervical cancer screening in the era of HPV vaccination. Vaccine. 2006;24(Suppl 3):171‐177. - PubMed
-
- Tota JE, Bentley J, Blake J, et al. Introduction of molecular HPV testing as the primary technology in cervical cancer screening: acting on evidence to change the current paradigm. Prev Med. 2017;98:5‐14. - PubMed
-
- Tota JE, Bentley J, Blake J, et al. Approaches for triaging women who test positive for human papillomavirus in cervical cancer screening. Prev Med. 2017;98:15‐20. - PubMed
