

Growth differentiation factor 15 as mortality predictor in heart failure patients with non-reduced ejection fraction
- PMID: 32589369
- PMCID: PMC7524215
- DOI: 10.1002/ehf2.12621
Growth differentiation factor 15 as mortality predictor in heart failure patients with non-reduced ejection fraction
Abstract
Aims: The prognostic value of biomarkers in patients with heart failure (HF) and mid-range (HFmrEF) or preserved ejection fraction (HFpEF) has not been widely addressed. The aim of this study was to assess whether the prognostic value of growth differentiation factor 15 (GDF-15) is superior to that of N-terminal pro-brain natriuretic peptide (NT-proBNP) in patients with HFmrEF or HFpEF.
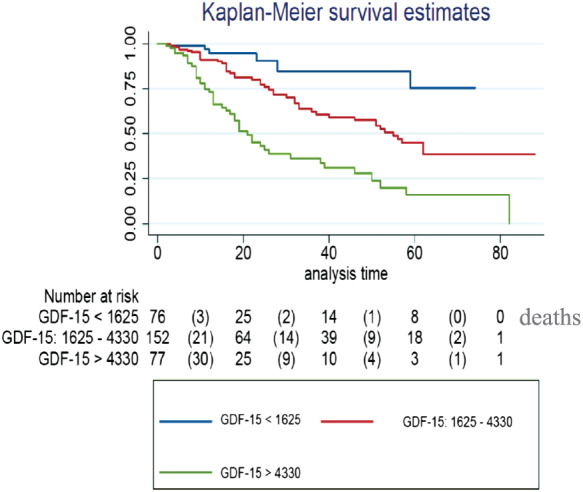
Methods and results: Heart failure patients with either HFpEF or HFmrEF were included in the study. During their first visit to the HF unit, serum samples were obtained and stored for later assessment of GDF-15 and NT-proBNP concentrations. Patients were followed up by the HF unit. The main endpoint was all-cause mortality. A total of 311 patients, 90 (29%) HFmrEF and 221 (71%) HFpEF, were included. Mean age was 72 ± 13 years, and 136 (44%) were women. No differences were found in GDF-15 or NT-proBNP concentrations between both HF groups. During a median follow-up of 15 months (Q1-Q3: 9-30 months), 98 patients (32%) died, most (71%) of cardiovascular causes. Patients who died had higher median concentrations of GDF-15 (4085 vs. 2270 ng/L, P < 0.0001) and NT-proBNP (1984 vs. 1095 ng/L, P < 0.0001). A Cox multivariable model identified New York Heart Association Functional Class III (P = 0.04), systolic blood pressure (P = 0.01), left atrial diameter (P = 0.03), age >65 years (P < 0.0001), and GDF-15 concentrations (P = 0.01) but not NT-proBNP as independent predictors of all-cause mortality. The area under the curve was 0.797 for the basic model including NT-proBNP, and the area under the curve comparing the overall model was 0.819, P = 0.016 (DeLong's test). Integrated discrimination improvement index after the inclusion of GDF-15 in the model with the mortality risk factors was 0.033; that is, the ability to predict death increased by 3.3% (P = 0.004). Net reclassification improvement was 0.548 (P < 0.001); that is, the capacity to improve the classification of the event (mortality) was 54.8%. GDF-15 concentrations were divided in tertiles (<1625, 1625-4330, and >4330 ng/L), and survival curves were evaluated using the Kaplan-Meier technique. Patients in the highest tertile had the poorest 5 year survival, at 16%, whereas the lowest tertile had the best survival, of 78% (P < 0.001).
Conclusions: Growth differentiation factor 15 was superior to NT-proBNP for assessing prognosis in patients with HFpEF and HFmrEF. GDF-15 emerges as a strong, independent biomarker for identifying HFmrEF and HFpEF patients with worse prognosis.
Keywords: Biomarkers; Chronic heart failure; GDF-15; HFmrEF; HFpEF.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Biomarkers for characterization of heart failure - Distinction of heart failure with preserved and reduced ejection fraction.Int J Cardiol. 2017 Jan 15;227:272-277. doi: 10.1016/j.ijcard.2016.11.110. Epub 2016 Nov 9. Int J Cardiol. 2017. PMID: 27838133
-
Prognostic value of growth differentiation factor-15 in heart failure among whole ejection fraction phenotypes.ESC Heart Fail. 2024 Aug;11(4):2295-2304. doi: 10.1002/ehf2.14807. Epub 2024 Apr 19. ESC Heart Fail. 2024. PMID: 38641904 Free PMC article.
-
Growth differentiation factor 15 in heart failure with preserved vs. reduced ejection fraction.Eur J Heart Fail. 2016 Jan;18(1):81-8. doi: 10.1002/ejhf.431. Epub 2015 Oct 25. Eur J Heart Fail. 2016. PMID: 26497848
-
Biomarkers and diagnostics in heart failure.Biochim Biophys Acta. 2013 Dec;1832(12):2442-50. doi: 10.1016/j.bbadis.2012.12.014. Epub 2013 Jan 9. Biochim Biophys Acta. 2013. PMID: 23313577 Review.
-
Validation of the MEDIA echo score for the prognosis of heart failure with preserved ejection fraction.Heart Fail Rev. 2023 Mar;28(2):453-464. doi: 10.1007/s10741-022-10266-2. Epub 2022 Aug 30. Heart Fail Rev. 2023. PMID: 36038694 Review.
Cited by
-
Prognostic value of Growth differentiation factors 15 in Acute heart failure patients with preserved ejection fraction.ESC Heart Fail. 2023 Apr;10(2):1025-1034. doi: 10.1002/ehf2.14271. Epub 2022 Dec 14. ESC Heart Fail. 2023. PMID: 36519216 Free PMC article.
-
A Meta-Analysis of Growth Differentiation Factor-15 and Prognosis in Chronic Heart Failure.Front Cardiovasc Med. 2021 Nov 5;8:630818. doi: 10.3389/fcvm.2021.630818. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34805295 Free PMC article.
-
GDF15 and Cardiac Cells: Current Concepts and New Insights.Int J Mol Sci. 2021 Aug 18;22(16):8889. doi: 10.3390/ijms22168889. Int J Mol Sci. 2021. PMID: 34445593 Free PMC article. Review.
-
Association between growth differentiation factor-15 and adverse outcomes among patients with heart failure: A systematic literature review.Heliyon. 2024 Aug 8;10(16):e35916. doi: 10.1016/j.heliyon.2024.e35916. eCollection 2024 Aug 30. Heliyon. 2024. PMID: 39229539 Free PMC article.
-
Mitochondrial stress and mitokines in aging.Aging Cell. 2023 Feb;22(2):e13770. doi: 10.1111/acel.13770. Epub 2023 Jan 15. Aging Cell. 2023. PMID: 36642986 Free PMC article. Review.
References
-
- Lam CSP, Solomon SD. The middle child in heart failure: heart failure with mid‐range ejection fraction (40–50%). Eur J Heart Fail 2014; 16: 1049–1055. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González‐Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, Authors/Task Force Members., Document Reviewers . 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur J Heart Fail 2016; 18: 891–975. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
