

Multimodal non-invasive assessment of intracranial hypertension: an observational study
- PMID: 32591024
- PMCID: PMC7318399
- DOI: 10.1186/s13054-020-03105-z
Multimodal non-invasive assessment of intracranial hypertension: an observational study
Abstract
Background: Although placement of an intra-cerebral catheter remains the gold standard method for measuring intracranial pressure (ICP), several non-invasive techniques can provide useful estimates. The aim of this study was to compare the accuracy of four non-invasive methods to assess intracranial hypertension.
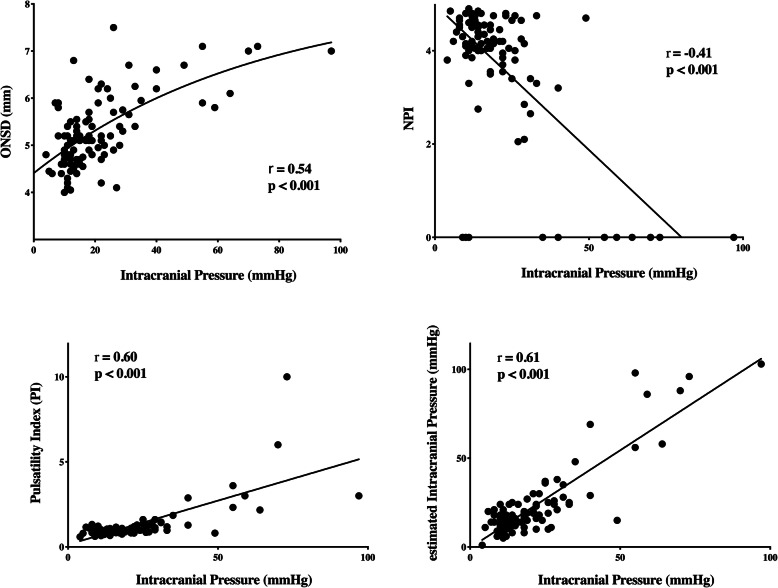
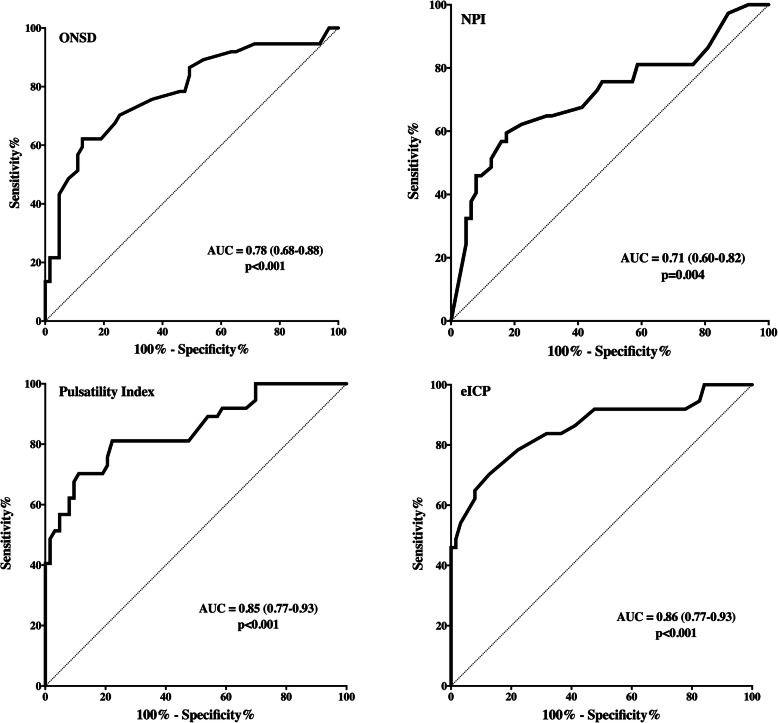
Methods: We reviewed prospectively collected data on adult intensive care unit (ICU) patients with traumatic brain injury (TBI), subarachnoid hemorrhage (SAH), or intracerebral hemorrhage (ICH) in whom invasive ICP monitoring had been initiated and estimates had been simultaneously collected from the following non-invasive indices: optic nerve sheath diameter (ONSD), pulsatility index (PI), estimated ICP (eICP) using transcranial Doppler, and the neurological pupil index (NPI) measured using automated pupillometry. Intracranial hypertension was defined as an invasively measured ICP > 20 mmHg.
Results: We studied 100 patients (TBI = 30; SAH = 47; ICH = 23) with a median age of 52 years. The median invasively measured ICP was 17 [12-25] mmHg and intracranial hypertension was present in 37 patients. Median values from the non-invasive techniques were ONSD 5.2 [4.8-5.8] mm, PI 1.1 [0.9-1.4], eICP 21 [14-29] mmHg, and NPI 4.2 [3.8-4.6]. There was a significant correlation between all the non-invasive techniques and invasive ICP (ONSD, r = 0.54; PI, r = 0.50; eICP, r = 0.61; NPI, r = - 0.41-p < 0.001 for all). The area under the curve (AUC) to estimate intracranial hypertension was 0.78 [CIs = 0.68-0.88] for ONSD, 0.85 [95% CIs 0.77-0.93] for PI, 0.86 [95% CIs 0.77-0.93] for eICP, and 0.71 [95% CIs 0.60-0.82] for NPI. When the various techniques were combined, the highest AUC (0.91 [0.84-0.97]) was obtained with the combination of ONSD with eICP.
Conclusions: Non-invasive techniques are correlated with ICP and have an acceptable accuracy to estimate intracranial hypertension. The multimodal combination of ONSD and eICP may increase the accuracy to estimate the occurrence of intracranial hypertension.
Keywords: Brain injury; Neuro-ICU; Non-invasive intracranial pressure; Optic nerve sheath diameter; Pupillometer.
Conflict of interest statement
None
Figures
References
-
- Carney N, Totten AM, O’Reilly C, Ullman JS, GWJ H, Bell MJ, et al. Guidelines for the management of severe traumatic brain injury, fourth edition. Neurosurgery. 2016;19:1. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
