

Kidney Disease, Intensive Hypertension Treatment, and Risk for Dementia and Mild Cognitive Impairment: The Systolic Blood Pressure Intervention Trial
- PMID: 32591439
- PMCID: PMC7461687
- DOI: 10.1681/ASN.2020010038
Kidney Disease, Intensive Hypertension Treatment, and Risk for Dementia and Mild Cognitive Impairment: The Systolic Blood Pressure Intervention Trial
Abstract
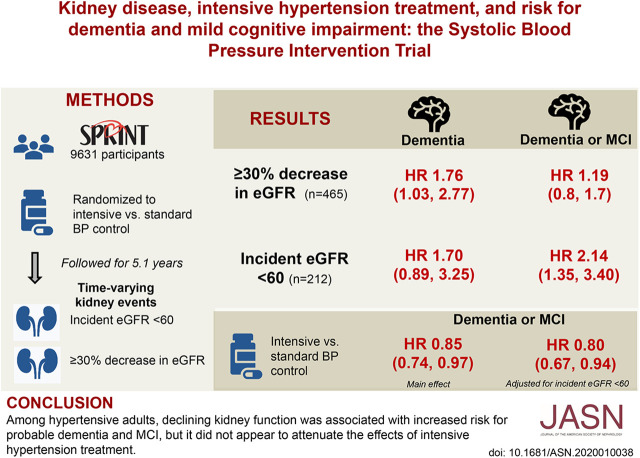
Background: Intensively treating hypertension may benefit cardiovascular disease and cognitive function, but at the short-term expense of reduced kidney function.
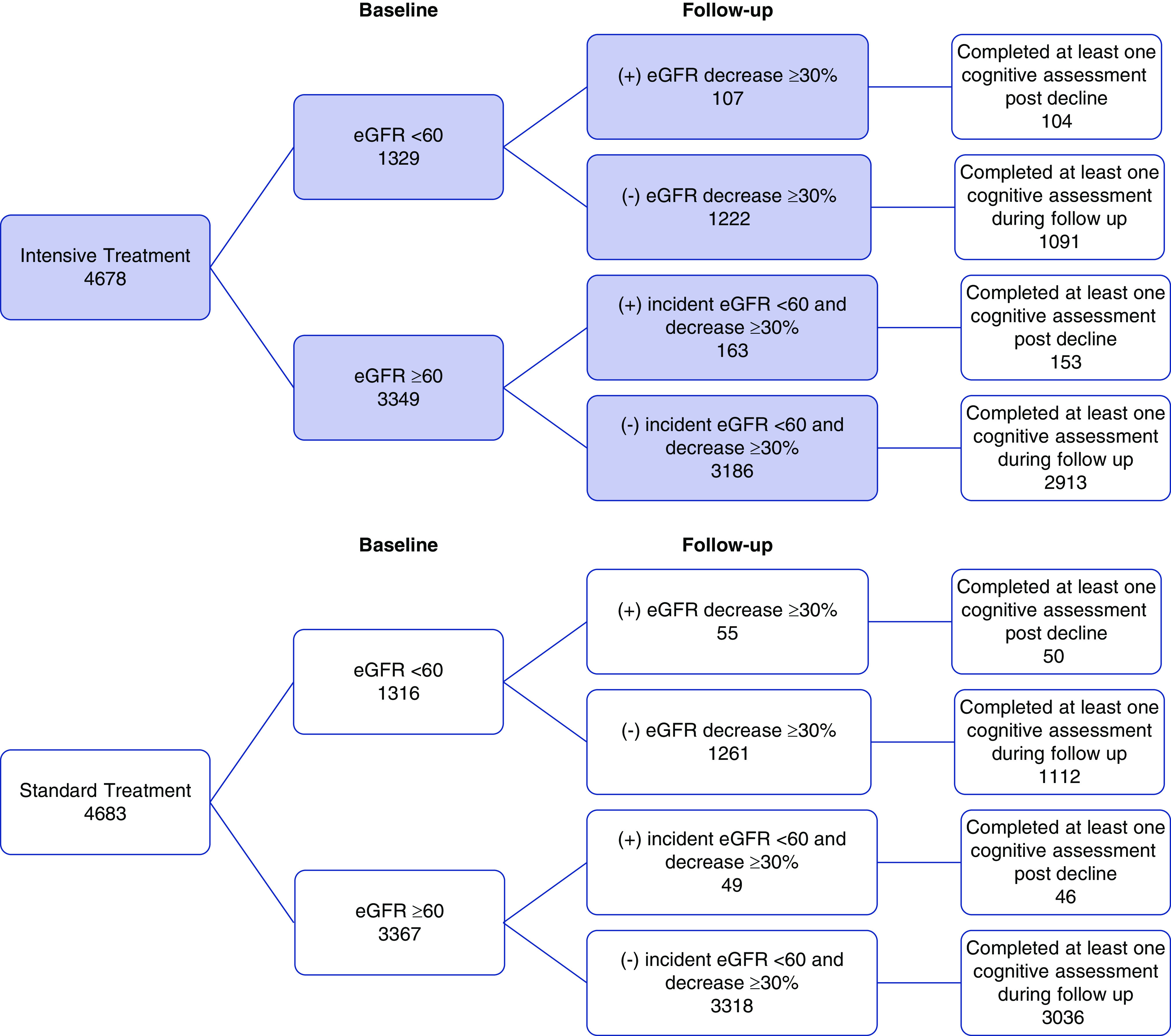
Methods: We investigated markers of kidney function and the effect of intensive hypertension treatment on incidence of dementia and mild cognitive impairment (MCI) in 9361 participants in the randomized Systolic Blood Pressure Intervention Trial, which compared intensive versus standard systolic BP lowering (targeting <120 mm Hg versus <140 mm Hg, respectively). We categorized participants according to baseline and longitudinal changes in eGFR and urinary albumin-to-creatinine ratio. Primary outcomes were occurrence of adjudicated probable dementia and MCI.
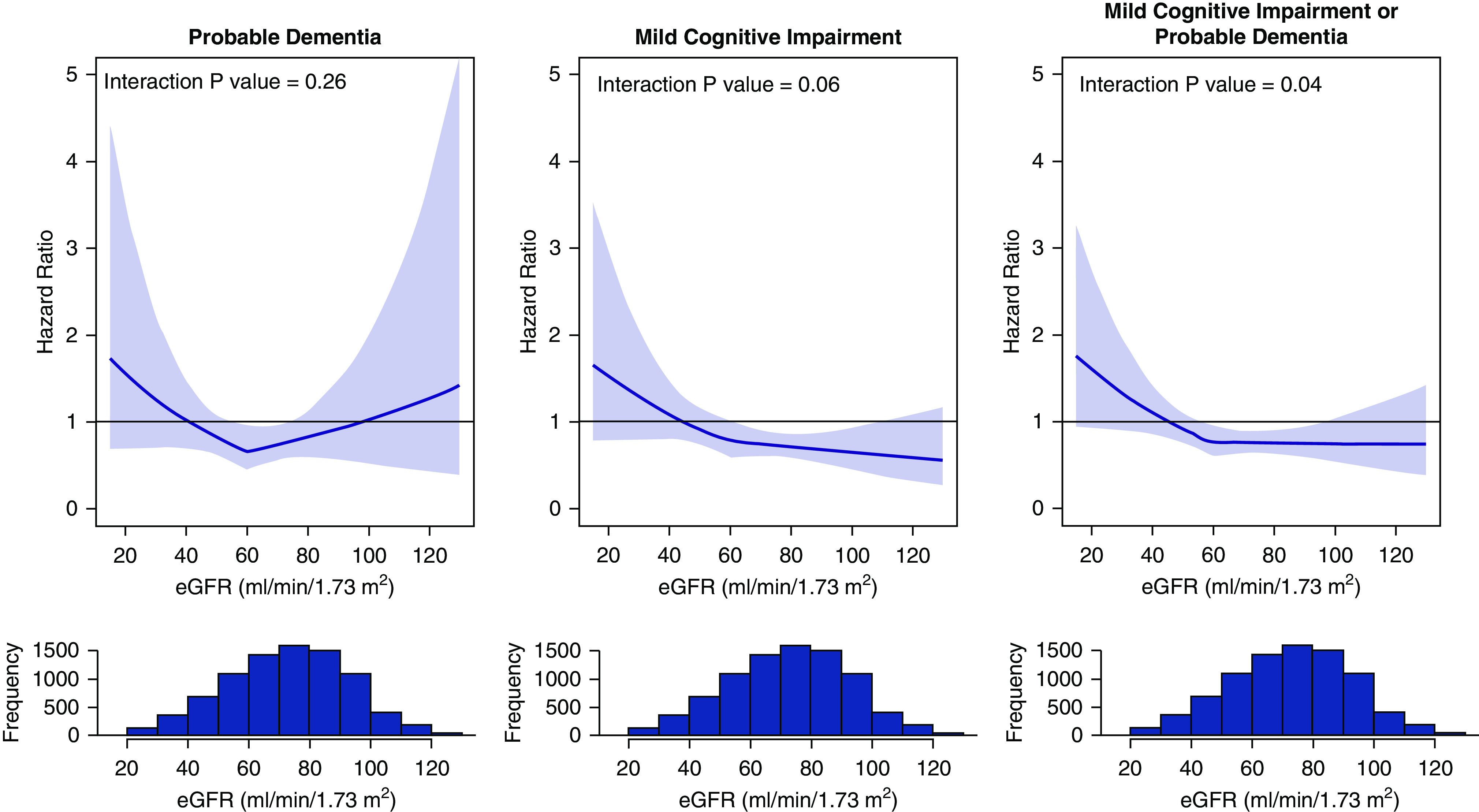
Results: Among 8563 participants who completed at least one cognitive assessment during follow-up (median 5.1 years), probable dementia occurred in 325 (3.8%) and MCI in 640 (7.6%) participants. In multivariable adjusted analyses, there was no significant association between baseline eGFR <60 ml/min per 1.73 m2 and risk for dementia or MCI. In time-varying analyses, eGFR decline ≥30% was associated with a higher risk for probable dementia. Incident eGFR <60 ml/min per 1.73 m2 was associated with a higher risk for MCI and a composite of dementia or MCI. Although these kidney events occurred more frequently in the intensive treatment group, there was no evidence that they modified or attenuated the effect of intensive treatment on dementia and MCI incidence. Baseline and incident urinary ACR ≥30 mg/g were not associated with probable dementia or MCI, nor did the urinary ACR modify the effect of intensive treatment on cognitive outcomes.
Conclusions: Among hypertensive adults, declining kidney function measured by eGFR is associated with increased risk for probable dementia and MCI, independent of the intensity of hypertension treatment.
Keywords: Epidemiology and outcomes; glomerular filtration rate; hypertension; systolic blood pressure.
Copyright © 2020 by the American Society of Nephrology.
Figures
Comment in
-
Authors' Reply.J Am Soc Nephrol. 2020 Dec;31(12):2966. doi: 10.1681/ASN.2020081189. Epub 2020 Sep 11. J Am Soc Nephrol. 2020. PMID: 32931447 Free PMC article. No abstract available.
-
A Single Point-in-Time eGFR Is Not Associated with Increased Risk of Dementia in the Elderly.J Am Soc Nephrol. 2020 Dec;31(12):2965. doi: 10.1681/ASN.2020081119. Epub 2020 Sep 11. J Am Soc Nephrol. 2020. PMID: 32936778 Free PMC article. No abstract available.
References
-
- Seliger SL, Siscovick DS, Stehman-Breen CO, Gillen DL, Fitzpatrick A, Bleyer A, et al.: Moderate renal impairment and risk of dementia among older adults: The cardiovascular health cognition study. J Am Soc Nephrol 15: 1904–1911, 2004. - PubMed
-
- Kurella M, Chertow GM, Fried LF, Cummings SR, Harris T, Simonsick E, et al.: Chronic kidney disease and cognitive impairment in the elderly: The health, aging, and body composition study. J Am Soc Nephrol 16: 2127–2133, 2005. - PubMed
-
- Fryar CDOY, Hales CM, Zhang G, Kruszon-Moran D: Hypertension prevalence and control among adults: United States, 2015-2016. NCHS Data Brief 289: 1–8, 2017 - PubMed
-
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr., Collins KJ, Dennison Himmelfarb C, et al.: 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: Executive summary: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines [published correction appears in Hypertension 72: e33, 2018]. Hypertension 71: 1269–1324, 2018. - PubMed
-
- Klahr S, Levey AS, Beck GJ, Caggiula AW, Hunsicker L, Kusek JW, et al.: Modification of Diet in Renal Disease Study Group : The effects of dietary protein restriction and blood-pressure control on the progression of chronic renal disease. N Engl J Med 330: 877–884, 1994. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1 TR000433/TR/NCATS NIH HHS/United States
- UL1 TR000445/TR/NCATS NIH HHS/United States
- UL1 TR000005/TR/NCATS NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- UL1 TR000064/TR/NCATS NIH HHS/United States
- UL1 TR000075/TR/NCATS NIH HHS/United States
- P30 AG049638/AG/NIA NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- HHSN268200900048C/HL/NHLBI NIH HHS/United States
- R01 AG055606/AG/NIA NIH HHS/United States
- P30 GM103337/GM/NIGMS NIH HHS/United States
- UL1 TR001064/TR/NCATS NIH HHS/United States
- HHSN268200900040C/HL/NHLBI NIH HHS/United States
- UL1 RR025752/RR/NCRR NIH HHS/United States
- UL1 RR025771/RR/NCRR NIH HHS/United States
- HHSN268200900049C/HL/NHLBI NIH HHS/United States
- HHSN268200900046C/HL/NHLBI NIH HHS/United States
- UL1 TR000093/TR/NCATS NIH HHS/United States
- R01 DK092241/DK/NIDDK NIH HHS/United States
- UL1 TR000050/TR/NCATS NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1 TR000073/TR/NCATS NIH HHS/United States
- UL1 RR025755/RR/NCRR NIH HHS/United States
- HHSN268200900047C/HL/NHLBI NIH HHS/United States
- UL1 TR000002/TR/NCATS NIH HHS/United States
- UL1 TR002240/TR/NCATS NIH HHS/United States
- UL1 TR000105/TR/NCATS NIH HHS/United States
- UL1 RR024134/RR/NCRR NIH HHS/United States
- UL1 TR003142/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
