

Quantitative chest CT analysis in COVID-19 to predict the need for oxygenation support and intubation
- PMID: 32591888
- PMCID: PMC7317888
- DOI: 10.1007/s00330-020-07013-2
Quantitative chest CT analysis in COVID-19 to predict the need for oxygenation support and intubation
Abstract
Objective: Lombardy (Italy) was the epicentre of the COVID-19 pandemic in March 2020. The healthcare system suffered from a shortage of ICU beds and oxygenation support devices. In our Institution, most patients received chest CT at admission, only interpreted visually. Given the proven value of quantitative CT analysis (QCT) in the setting of ARDS, we tested QCT as an outcome predictor for COVID-19.
Methods: We performed a single-centre retrospective study on COVID-19 patients hospitalised from January 25, 2020, to April 28, 2020, who received CT at admission prompted by respiratory symptoms such as dyspnea or desaturation. QCT was performed using a semi-automated method (3D Slicer). Lungs were divided by Hounsfield unit intervals. Compromised lung (%CL) volume was the sum of poorly and non-aerated volumes (- 500, 100 HU). We collected patient's clinical data including oxygenation support throughout hospitalisation.
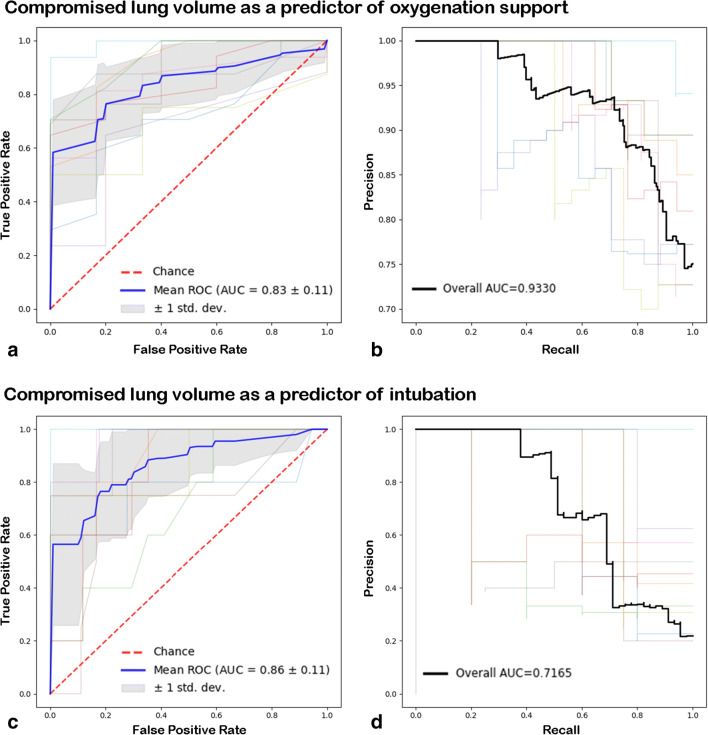
Results: Two hundred twenty-two patients (163 males, median age 66, IQR 54-6) were included; 75% received oxygenation support (20% intubation rate). Compromised lung volume was the most accurate outcome predictor (logistic regression, p < 0.001). %CL values in the 6-23% range increased risk of oxygenation support; values above 23% were at risk for intubation. %CL showed a negative correlation with PaO2/FiO2 ratio (p < 0.001) and was a risk factor for in-hospital mortality (p < 0.001).
Conclusions: QCT provides new metrics of COVID-19. The compromised lung volume is accurate in predicting the need for oxygenation support and intubation and is a significant risk factor for in-hospital death. QCT may serve as a tool for the triaging process of COVID-19.
Key points: • Quantitative computer-aided analysis of chest CT (QCT) provides new metrics of COVID-19. • The compromised lung volume measured in the - 500, 100 HU interval predicts oxygenation support and intubation and is a risk factor for in-hospital death. • Compromised lung values in the 6-23% range prompt oxygenation therapy; values above 23% increase the need for intubation.
Keywords: COVID-19; Intubation; Pulmonary ventilation; Tomography, spiral computed.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures



References
-
- Situation update for the EU/EEA and the UK, as of 27 March 2020. https://www.ecdc.europa.eu/en/cases-2019-ncov-eueea. Accessed 28 Mar 2020
-
- Poston JT, Patel BK, Davis AM (2020) Management of critically ill adults with COVID-19. JAMA. 10.1001/jama.2020.4914 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
