

Circulating troponin and further left ventricular ejection fraction improvement in patients with previously recovered left ventricular ejection fraction
- PMID: 32592541
- PMCID: PMC7524210
- DOI: 10.1002/ehf2.12863
Circulating troponin and further left ventricular ejection fraction improvement in patients with previously recovered left ventricular ejection fraction
Abstract
Aims: The aim of this study is to determine factors associated with long-term recovery of left ventricular ejection fraction (LVEF) in patients with heart failure with reduced EF (HFrEF) and if further recovery also occurs in this group.
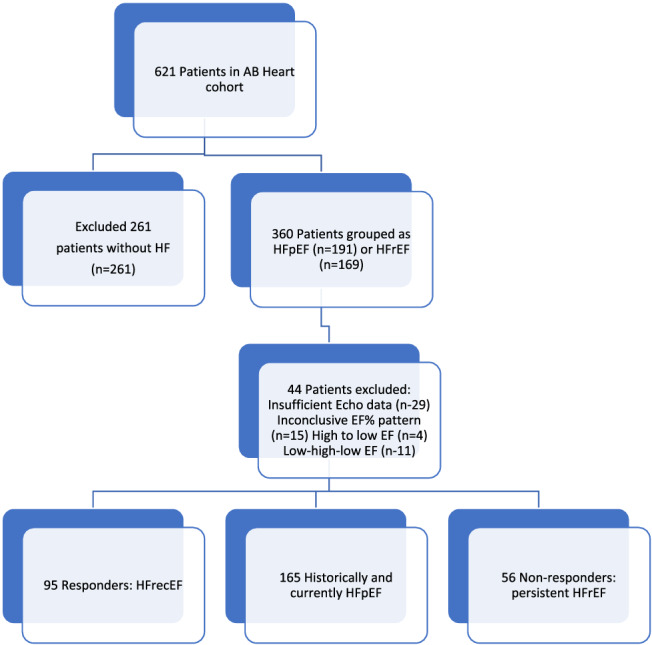
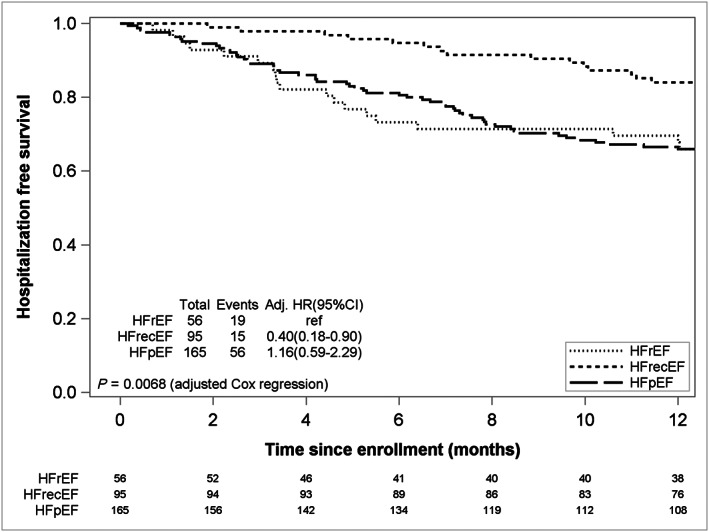
Methods and results: Among 621 participants enrolled in the Alberta Heart Failure Etiology and Analysis Team (HEART) Study, 316 with Stage C HF underwent comprehensive imaging and biomarker testing at enrolment and at 1-year follow up. Using pre-enrolment data, HF with recovered EF (HFrecEF) was defined as an absolute improvement ≥5% in LVEF from the prior lowest LVEF value, with a final LVEF value > 35% at or prior to study baseline. Participants with all LVEF > 40% were included for comparison. Hospitalization-free survival to 5 years was performed. The median cohort age was 66 years, and time from diagnosis was 4 years; 82% were male patients. Of the 316 patients, 95 (30%) patients had HFrecEF and 56 (18%) patients pHFrEF. On multivariate analysis, only shorter duration of HF was predictive of HFrecEF status. Over 1 year, LVEF increased in the HFrecEF group 4.0% (0.15-7.90, P = 0.042) as compared with persistent HFrEF, who in turn demonstrated higher baseline serum high sensitivity Troponin-T with further increase at follow up 0.55(0.33-0.86, P = 0.011). No change in any parameter in the HFpEF/HFmrEF group at follow up was observed.
Conclusions: Patients with HFrecEF demonstrate evidence of additional late improvement in LVEF and unchanged troponin levels, in contrast to those with persistent HFrEF, where LVEF does not improve and serum troponin rises over time. These data help to inform mechanisms relating to late LV remodelling.
Keywords: Biomarkers; Heart failure; Left ventricular remodelling; Troponin.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- Aimo A, Gaggin HK, Barison A, Emdin M, Januzzi JL Jr. Imaging, biomarker, and clinical predictors of cardiac remodeling in heart failure with reduced ejection fraction. JACC Heart Fail 2019; 7: 782–794. - PubMed
-
- Punnoose LR, Givertz MM, Lewis EF, Pratibhu P, Stevenson LW, Desai AS. Heart failure with recovered ejection fraction: a distinct clinical entity. J Card Fail 2011; 17: 527–532. - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJV, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WHW, Tsai EJ, Wilkoff BL. 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013; 128: 1810–1852. - PubMed
-
- Ezekowitz JA, O'Meara E, McDonald MA, Abrams H, Chan M, Ducharme A, Giannetti N, Grzeslo A, Hamilton PG, Heckman GA, Howlett JG, Koshman SL, Lepage S, McKelvie RS, Moe GW, Rajda M, Swiggum E, Virani SA, Zieroth S, Al‐Hesayen A, Cohen‐Solal A, De D'Astous S, Estrella‐Holder E, Fremes S, Green L, Haddad H, Harkness K, Hernandez AF, Kouz S, LeBlanc M‐H, Masoudi FA, Ross HJ, Roussin A, Sussex B. 2017 comprehensive update of the Canadian Cardiovascular Society Guidelines for the management of heart failure. Can J Cardiol 2017; 33: 1342–1433. - PubMed
-
- Lupon J, Diez‐Lopez C, de Antonio M, Domingo M, Zamora E, Moliner P, González B, Santesmases J, Troya MI, Bayés‐Genís A. Recovered heart failure with reduced ejection fraction and outcomes: a prospective study. Eur J Heart Fail 2017; 19: 1615–1623. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous