

Multi-domain potential biomarkers for post-traumatic stress disorder (PTSD) severity in recent trauma survivors
- PMID: 32594097
- PMCID: PMC7320966
- DOI: 10.1038/s41398-020-00898-z
Multi-domain potential biomarkers for post-traumatic stress disorder (PTSD) severity in recent trauma survivors
Abstract
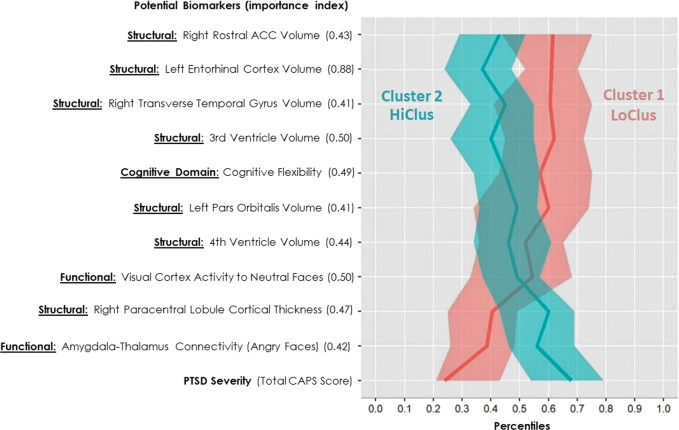
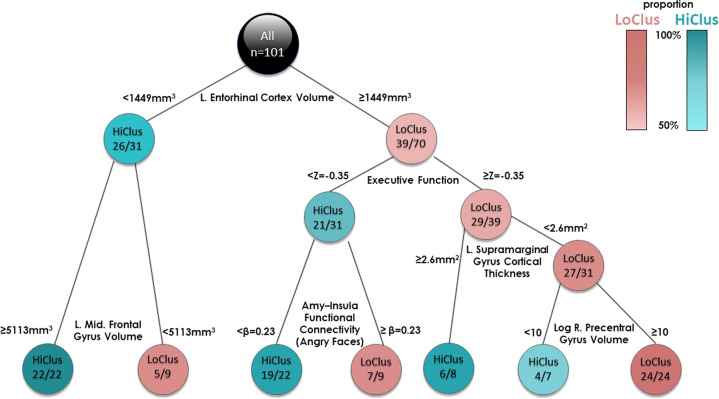
Contemporary symptom-based diagnosis of post-traumatic stress disorder (PTSD) largely overlooks related neurobehavioral mechanisms and relies entirely on subjective interpersonal reporting. Previous studies associating biomarkers with PTSD have mostly used symptom-based diagnosis as the main outcome measure, disregarding the wide variability and richness of PTSD phenotypical features. Here, we aimed to computationally derive potential biomarkers that could efficiently differentiate PTSD subtypes among recent trauma survivors. A three-staged semi-unsupervised method ("3C") was used to firstly categorize individuals by current PTSD symptom severity, then derive clusters based on clinical features related to PTSD (e.g. anxiety and depression), and finally to classify participants' cluster membership using objective multi-domain features. A total of 256 features were extracted from psychometrics, cognitive functioning, and both structural and functional MRI data, obtained from 101 adult civilians (age = 34.80 ± 11.95; 51 females) evaluated within 1 month of trauma exposure. The features that best differentiated cluster membership were assessed by importance analysis, classification tree, and ANOVA. Results revealed that entorhinal and rostral anterior cingulate cortices volumes (structural MRI domain), in-task amygdala's functional connectivity with the insula and thalamus (functional MRI domain), executive function and cognitive flexibility (cognitive testing domain) best differentiated between two clusters associated with PTSD severity. Cross-validation established the results' robustness and consistency within this sample. The neural and cognitive potential biomarkers revealed by the 3C analytics offer objective classifiers of post-traumatic morbidity shortly following trauma. They also map onto previously documented neurobehavioral mechanisms associated with PTSD and demonstrate the usefulness of standardized and objective measurements as differentiating clinical sub-classes shortly after trauma.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Perkonigg A, et al. Longitudinal course of posttraumatic stress disorder and posttraumatic stress disorder symptoms in a community sample of adolescents and young adults. Am. J. Psychiatry. 2005;162:1320–1327. - PubMed
-
- Blake DD, et al. The development of a Clinician-Administered PTSD Scale. J. Trauma Stress. 1995;8:75–90. - PubMed
-
- Keane TM, Kaloupek DG. Comorbid psychiatric disorders in PTSD. Ann. N. Y. Acad. Sci. 1997;821:24–34. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
