

The Safety of Delayed Versus Immediate Antibiotic Prescribing for Upper Respiratory Tract Infections
- PMID: 32594104
- PMCID: PMC8282258
- DOI: 10.1093/cid/ciaa890
The Safety of Delayed Versus Immediate Antibiotic Prescribing for Upper Respiratory Tract Infections
Abstract
Background: This study aimed to evaluate the clinical safety of delayed antibiotic prescribing for upper respiratory tract infections (URTIs), which is recommended in treatment guidelines for less severe cases.
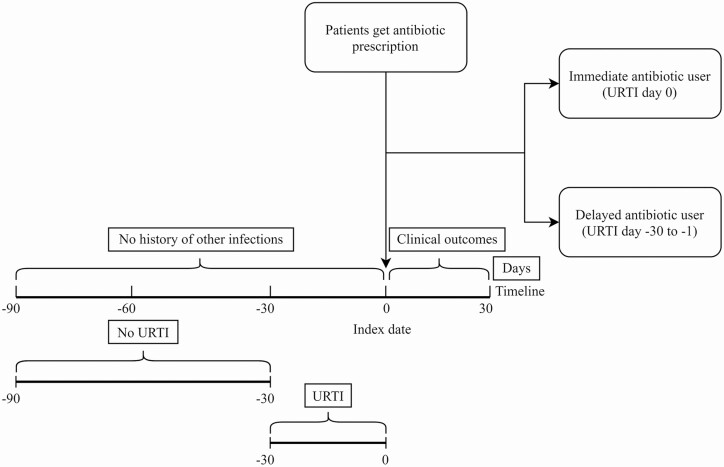
Methods: Two population-based cohort studies used the English Clinical Practice Research Databank and Welsh Secure Anonymized Information Linkage, containing electronic health records from primary care linked to hospital admission records. Patients with URTI and prescriptions of amoxicillin, clarithromycin, doxycycline, erythromycin, or phenoxymethylpenicillin were identified. Patients were stratified according to delayed and immediate prescribing relative to URTI diagnosis. Outcome of interest was infection-related hospital admission after 30 days.
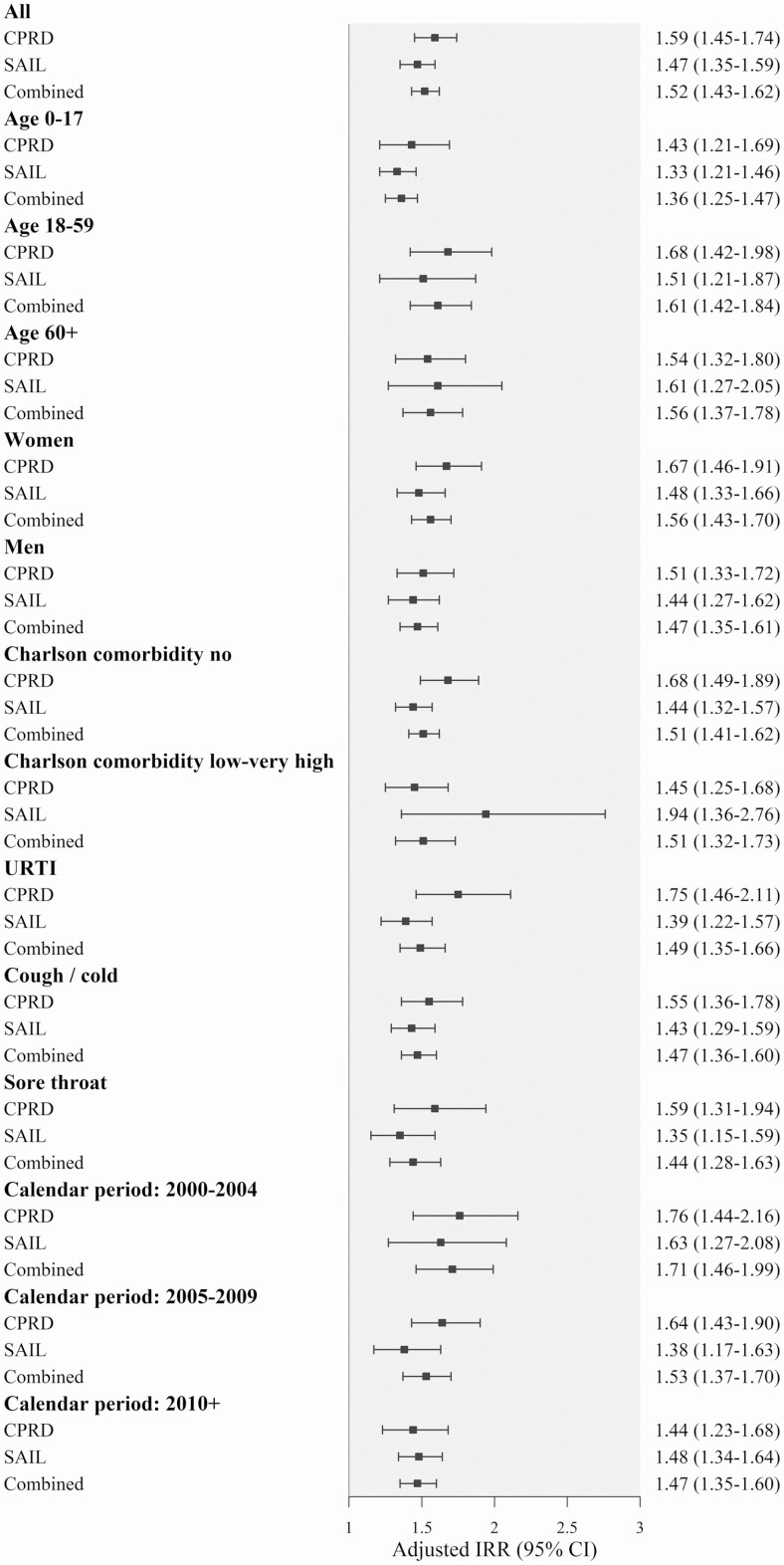
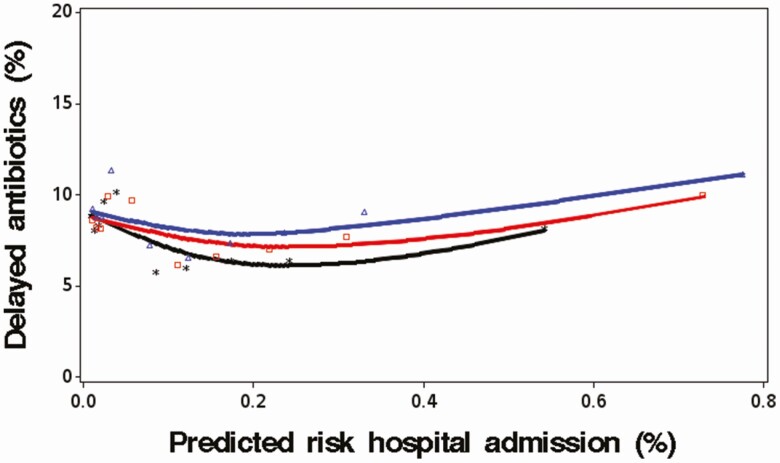
Results: The population included 1.82 million patients with an URTI and antibiotic prescription; 91.7% had an antibiotic at URTI diagnosis date (immediate) and 8.3% had URTI diagnosis in 1-30 days before (delayed). Delayed antibiotic prescribing was associated with a 52% increased risk of infection-related hospital admissions (adjusted hazard ratio, 1.52; 95% confidence interval, 1.43-1.62). The probability of delayed antibiotic prescribing was unrelated to predicted risks of hospital admission. Analyses of the number needed to harm showed considerable variability across different patient groups (median with delayed antibiotic prescribing, 1357; 2.5% percentile, 295; 97.5% percentile, 3366).
Conclusions: This is the first large population-based study examining the safety of delayed antibiotic prescribing. Waiting to treat URTI was associated with increased risk of hospital admission, although delayed antibiotic prescribing was used similarly between high- and low-risk patients. There is a need to better target delayed antibiotic prescribing to URTI patients with lower risks of complications.
Keywords: antibiotics; effectiveness; epidemiology; primary care; upper respiratory tract infections.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- Petersen I, Hayward AC, SACAR Surveillance Subgroup . Antibacterial prescribing in primary care. J Antimicrob Chemother 2007; 60(Suppl. 1):i43–7. Available at: http://academic.oup.com/jac/article/60/suppl_1/i43/999396/Antibacterial-.... Accessed 2 June 2019. - PubMed
-
- O’Neill J; on behalf of the Review on Antimicrobial Resistance. Tackling drug resistant-infection globally: final report and recommendations. Available at: https://amr-review.org/sites/default/files/160518_Finalpaper_withcover.pdf. Accessed 8 March 2018.
-
- Royal College of General Practitioners. TARGET Antibiotic Toolkit. Available at: https://www.rcgp.org.uk/TARGETantibiotics. Accessed 10 February 2019.
-
- National Institute of Health and Care Excellence. Overview | Respiratory tract infections (self-limiting): prescribing antibiotics | Guidance | NICE. Available at: https://www.nice.org.uk/guidance/cg69. Accessed 30 May 2019. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
