

Psychosocial burden of healthcare professionals in times of COVID-19 - a survey conducted at the University Hospital Augsburg
- PMID: 32595421
- PMCID: PMC7314868
- DOI: 10.3205/000281
Psychosocial burden of healthcare professionals in times of COVID-19 - a survey conducted at the University Hospital Augsburg
Abstract
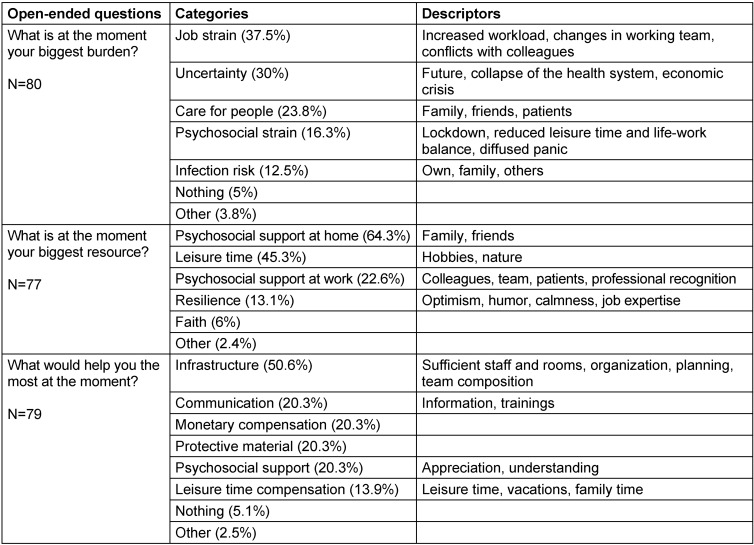
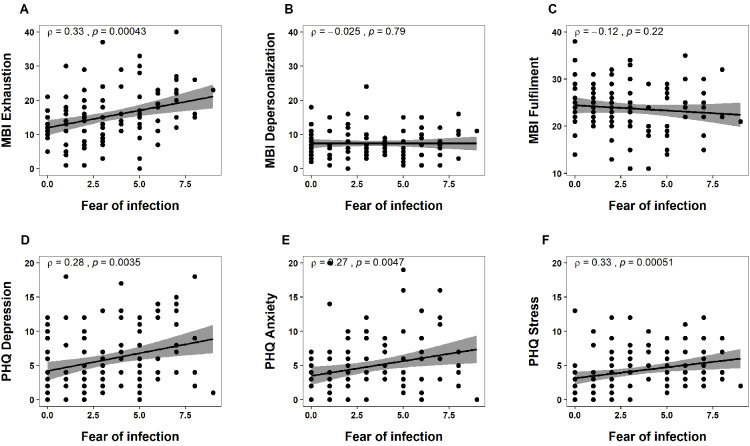
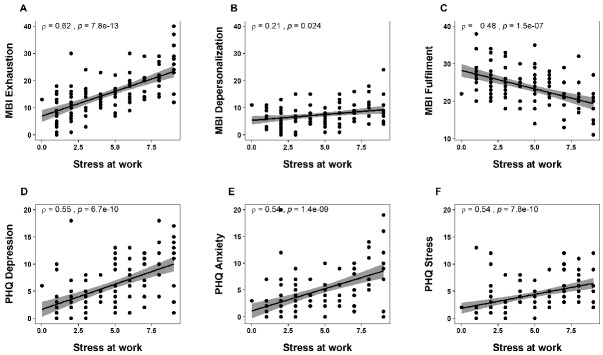
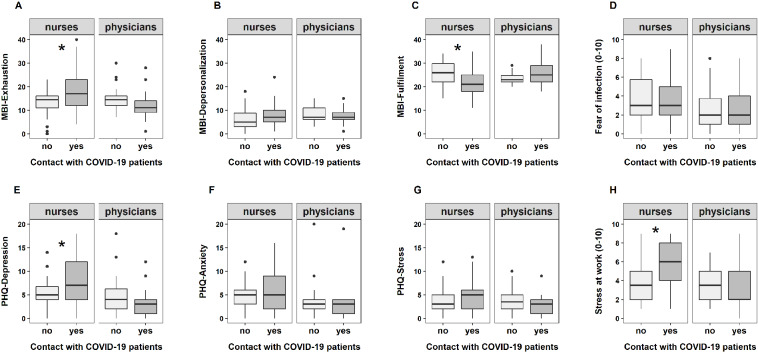
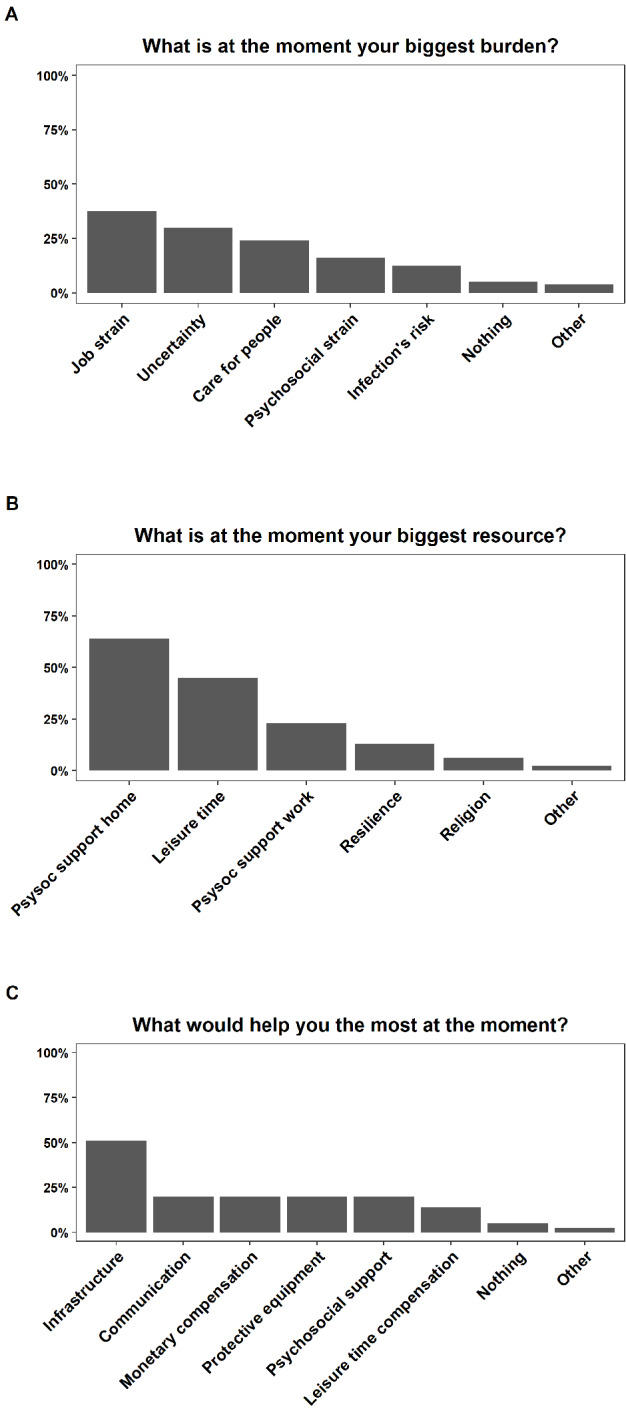
Objective: The outbreak of COVID-19 was declared a pandemic by the WHO in March 2020. Studies from China, where the virus first spread, have reported increased psychological strain in healthcare professionals. The aim of this study was to investigate the psychosocial burden of physicians and nurses depending on their degree of contact with COVID-19 patients. In addition, we explored which supportive resources they used and which supportive needs they experienced during the crisis. Methods: Data were collected between March and April 2020 at the University Hospital Augsburg. A total of 75 nurses and 35 physicians, working either in a special COVID-19 ward or in a regular ward, took part in the survey. The participants filled in two standardized questionnaires (the Patient Health Questionnaire, PHQ; and the Maslach Burnout Inventory, MBI), and reported their fear of a COVID-19 infection and stress at work on a 10-point Likert scale. Finally, they answered three open-ended questions about causes of burden, supportive resources and needs during the crisis. Results: Nurses working in the COVID-19 wards reported higher levels of stress, exhaustion, and depressive mood, as well as lower levels of work-related fulfilment compared to their colleagues in the regular wards. Physicians reported similar scores independent of their contact with COVID-19 patients. The most common causes for burden were job strain and uncertainty about the future. Psychosocial support as well as leisure time were listed as important resources, and a better infrastructure adjustment to COVID-19 at the hospital (e.g. sufficient staff, keeping teams and working schedules stable) as suggestion for improvement. Conclusions: Our findings indicate that especially nurses working in COVID-19 wards are affected psychologically by the consequences of the pandemic. This might be due to a higher workload and longer time in direct contact with COVID-19 patients, compared to physicians.
Ziel: Im März 2020 wurde der Ausbruch von COVID-19 von der WHO zur Pandemie erklärt, nachdem sich der Virus zunächst vor allem in China ausbreitete. Erste Studien berichteten von einer erhöhten psychologischen Belastung der Beschäftigten im chinesischen Gesundheitssystem. Das Ziel der vorliegenden Studie war es, die besonderen psychosozialen Belastungen von Ärztinnen und Ärzten im Vergleich zu Pflegerinnen und Pflegern durch COVID-19 zu erfassen, unter Berücksichtigung des Ausmaßes der Exposition zu COVID-19-Patientinnen und -Patienten. Zusätzlich wollten wir besonders relevante Ressourcen und Möglichkeiten zur Entlastung eruieren.Methoden: Die Datenerhebung erfolgte zwischen März und April 2020 am Universitätsklinikum Augsburg. Insgesamt nahmen 75 Pflegerinnen und Pfleger sowie 35 Ärztinnen und Ärzte an der Untersuchung teil, die entweder in regulären oder speziellen COVID-19-Stationen tätig waren. Neben zwei Standardinstrumenten (Gesundheitsfragebogen PHQ und Fragebogen zur Arbeitsbelastung MBI) bewerteten die Teilnehmenden ihre Angst, sich mit COVID-19 zu infizieren, und das Ausmaß der Belastung am Arbeitsplatz auf 10-stufigen numerischen Ratingskalen. Zusätzlich wurden drei offene Fragen zu den größten Belastungen, Ressourcen und Bedürfnissen durch bzw. in der Krise beantwortet.Ergebnisse: Insbesondere Pflegerinnen und Pfleger auf COVID-19-Stationen berichteten mehr Stress, Ermüdung, depressive Symptome und geringere Erfüllung am Arbeitsplatz als ihre Kolleginnen und Kollegen auf den regulären Stationen. Ärztinnen und Ärzte hingegen erzielten unabhängig von der spezifischen Exposition zu COVID-19-Patientinnen und -Patienten ähnliche Ergebnisse. Am häufigsten wurden von den Teilnehmenden das Arbeitspensum und die Ungewissheit hinsichtlich der weiteren Entwicklung als Ursache ihrer Belastung benannt. Psychosoziale Unterstützung und Freizeit wurden als wichtige Ressourcen aufgelistet. Die Teilnehmenden mahnten u.a. an, auf ausreichendes Personal, Kontinuität der Teamzusammensetzung und Schichtplanung zu achten.Schlussfolgerungen: Unsere Ergebnisse zeigen, dass insbesondere das Pflegepersonal – im Kontrast zu Ärztinnen und Ärzten – auf COVID-19-Stationen psychosozial unter den Folgen der Pandemie leidet, vermutlich als Konsequenz der Mehrarbeit und des höheren Expositionsrisikos.
Keywords: COVID-19; health personnel; health resources; mental health; psychological burnout.
Copyright © 2020 Zerbini et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
