

The advantage of cone-beam computerized tomography over panoramic radiography and temporomandibular joint quadruple radiography in assessing temporomandibular joint osseous degenerative changes
- PMID: 32595895
- PMCID: PMC7305453
- DOI: 10.1016/j.jds.2020.03.004
The advantage of cone-beam computerized tomography over panoramic radiography and temporomandibular joint quadruple radiography in assessing temporomandibular joint osseous degenerative changes
Abstract
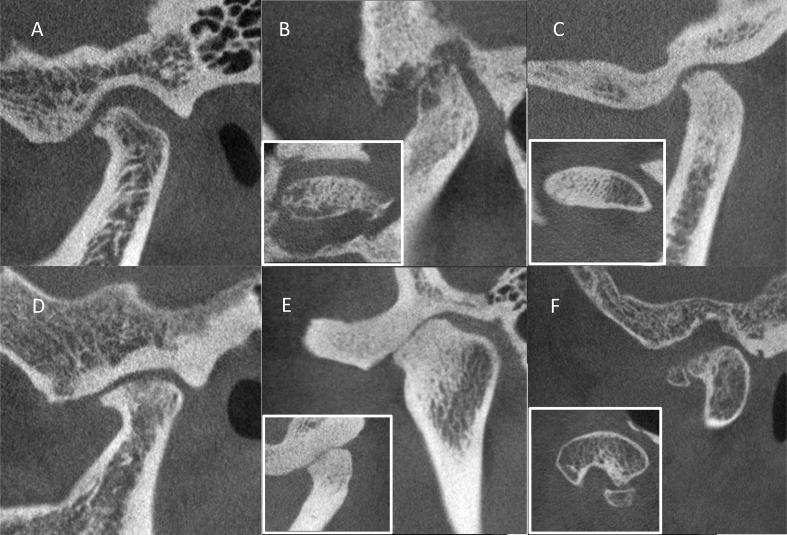
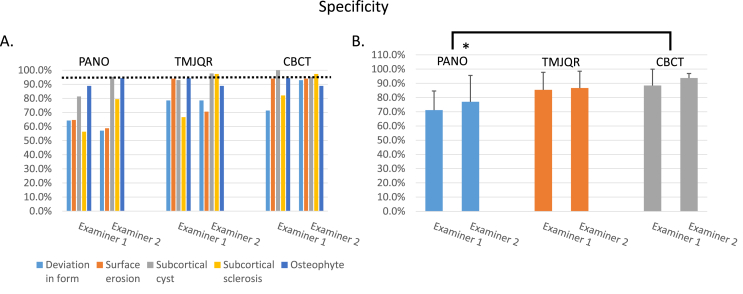
Background/purpose: The clinical diagnosis of temporomandibular joint (TMJ) degenerative joint disease (DJD) is based primarily on radiographic features of the condyle and articular eminence. The purpose of this study was to compare the reliability, sensitivity, and specificity of using plain radiography to that of cone-beam computerized tomography (CBCT) in identifying different types of osseous degenerative features in the TMJ condyle.
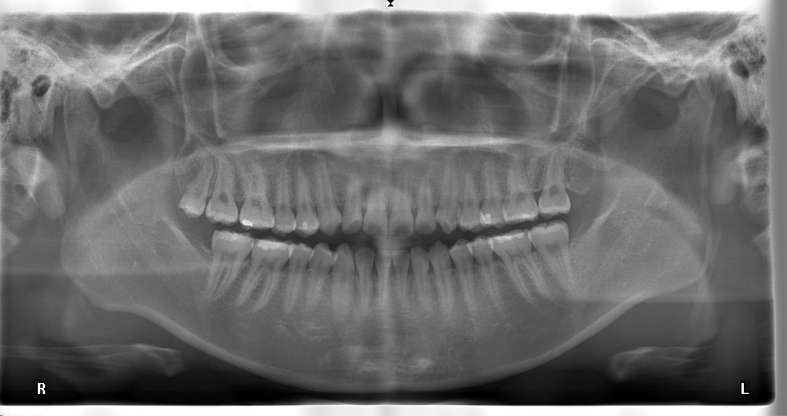
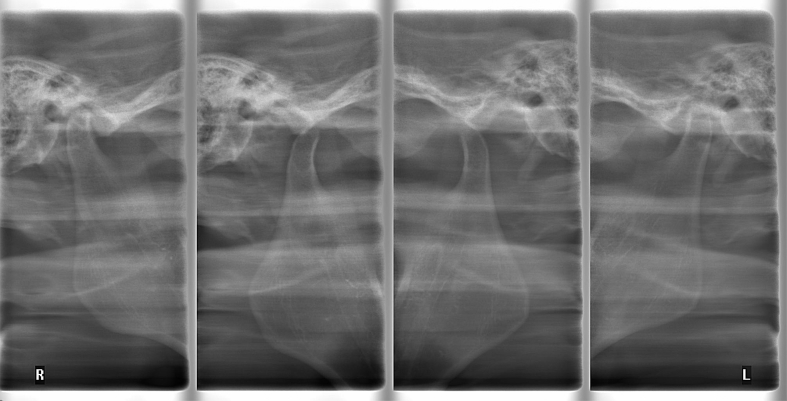
Materials and methods: The panoramic radiography (PANO), TMJ quadruple radiography (TMJQR) and CBCT images of 29 patients' TMJs were retrieved from a computer database and independently evaluated by a young oral surgeon and a senior TMD specialist. The examiners diagnosed osseous degenerative features on the radiographic images. The radiologist-assisted CBCT diagnoses were used as a reference standard and the reliability, sensitivity, and specificity of using the three radiographic modalities were statistically analyzed.
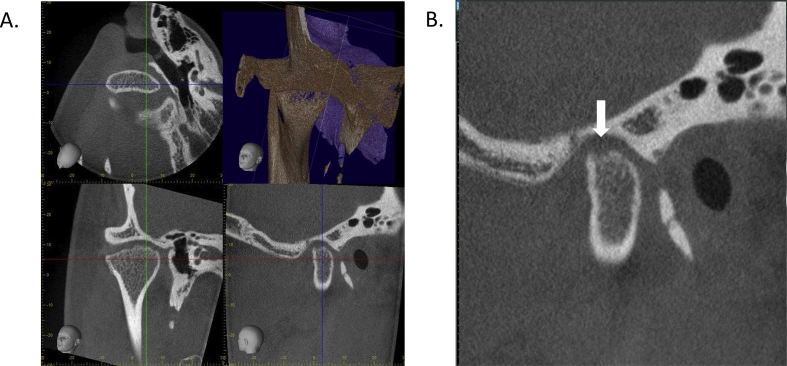
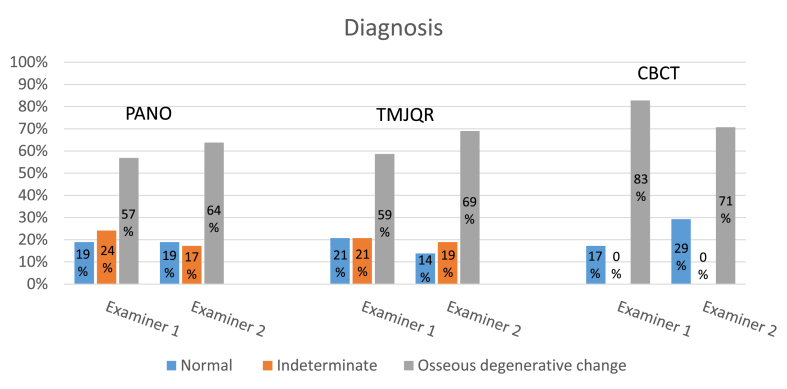
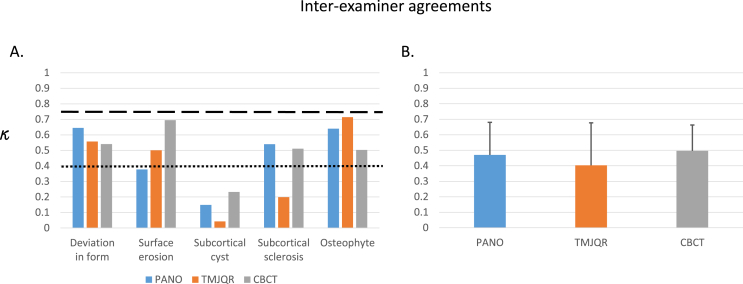
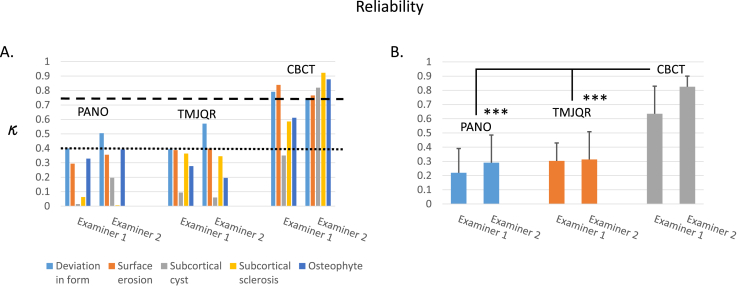
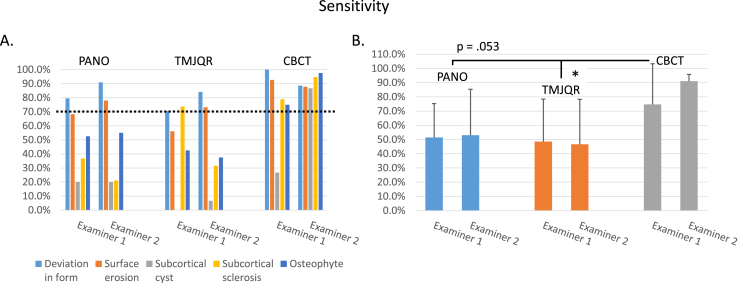
Results: There were cases of indeterminate diagnoses using the PANO and TMJQR due to superimposition from surrounding structures, but none using CBCT. Reliability was generally poor when using PANO and TMJQR for detecting osseous degenerative features of the TMJ condyle but good to excellent when using CBCT. The sensitivity and specificity in the use of PANO and TMJQR were typically below acceptable, but the levels were generally satisfactory when using CBCT.
Conclusion: CBCT is superior to plain radiographic modalities for diagnosing osseous degenerative features of TMJs with regard to indeterminate cases, reliability, sensitivity, and specificity. It is recommended that CBCT can be used as an effective tool in identifying TMJ osteoarthritis.
Keywords: Cone-beam computerized tomography; Osseous degenerative features; Panoramic radiography; TMJ; TMJ quadruple Radiography.
© 2020 Association for Dental Sciences of the Republic of China. Publishing services by Elsevier B.V.
Figures
References
-
- Laskin D., Greenfield W., Gale E. The President's conference on the examination, diagnosis and management of temporomandibular disorders. Chicago: American Dental Association.Kopp S. Topographical distribution of sulfated glycosaminoglycans in the surface layers of the human temporomandibular joint. J Oral Pathol. 1983;7:283–294. - PubMed
-
- Schiffman E., Ohrbach R., Truelove E. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and Research applications: recommendations of the international RDC/TMD consortium network and orofacial pain special interest group. J Oral Facial Pain Headache. 2014;28:6–27. - PMC - PubMed
-
- Jiao K., Niu L.N., Wang M.Q. Subchondral bone loss following orthodontically induced cartilage degradation in the mandibular condyles of rats. Bone. 2011;48:362–371. - PubMed
LinkOut - more resources
Full Text Sources
