

Endoscopic endonasal intraconal orbit surgery
- PMID: 32596654
- PMCID: PMC7296506
- DOI: 10.1016/j.wjorl.2019.07.001
Endoscopic endonasal intraconal orbit surgery
Abstract
Endoscopic endonasal orbital surgery is evolving. With increasing knowledge, expertise, and technology, the historical limits of the endonasal endoscopic approach to the orbit have been redefined. This review discusses the clinical presentation and etiology, and highlights the pertinent anatomy, and discusses the diagnostic workup and surgical approach to orbital tumors and post-operative care. The role of the multidisciplinary team is not to be underestimated. The introduction of a classification system to ensure standardization of technical difficulty and outcome data will assist with international collaboration and further consolidate our attainment of knowledge in this developing field.
Keywords: Endoscopic endonasal orbital surgery; Extraconal space tumors; Intraconal space tumors; Orbital cavernous hemangioma.
© 2019 The Authors.
Figures





References
-
- Shields J.A., Shields C.L., Scartozzi R. Survey of 1264 patients with orbital tumors and simulating lesions: the 2002 Montgomery Lecture, part 1. Ophthalmology. 2004;111:997–1008. - PubMed
-
- Bleier B.S., Castelnuovo P., Battaglia P. Endoscopic endonasal orbital cavernous hemangioma resection: global experience in techniques and outcomes. Int Forum Allergy Rhinol. 2016;6:156–161. - PubMed
-
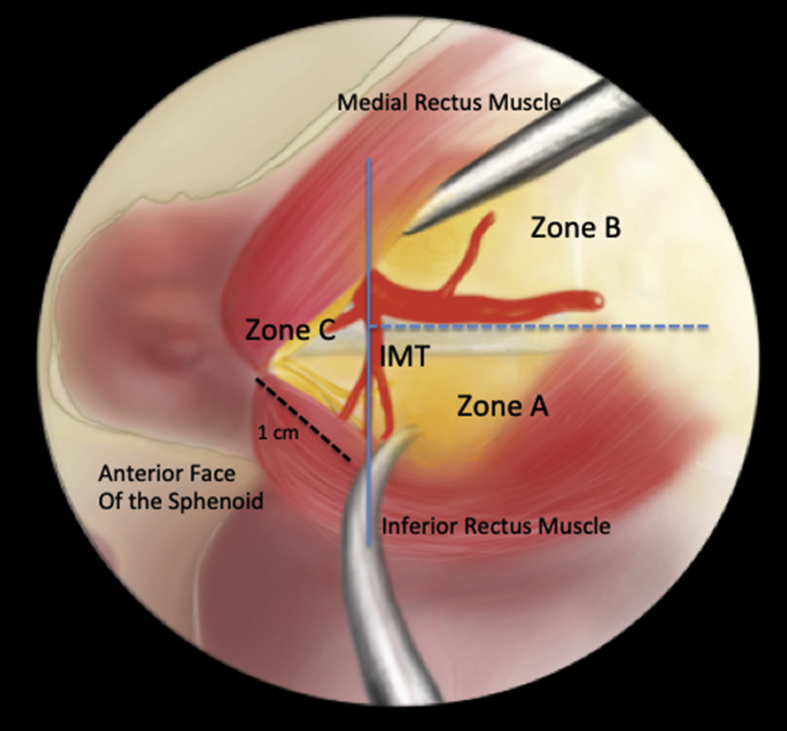
- Bleier B.S., Healy D.Y., Chhabra N., Freitag S. Compartmental endoscopic surgical anatomy of the medial intraconal orbital space. Int Forum Allergy Rhinol. 2014;4:587–591. - PubMed
-
- Perrini P., Cardia A., Fraser K., Lanzino G. A microsurgical study of the anatomy and course of the ophthalmic artery and its possibly dangerous anastomoses. J Neurosurg. 2007;106:142–150. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
