

Remote ischaemic preconditioning ameliorates anthracycline-induced cardiotoxicity and preserves mitochondrial integrity
- PMID: 32597960
- PMCID: PMC7983009
- DOI: 10.1093/cvr/cvaa181
Remote ischaemic preconditioning ameliorates anthracycline-induced cardiotoxicity and preserves mitochondrial integrity
Abstract
Aims: Anthracycline-induced cardiotoxicity (AIC) is a serious adverse effect among cancer patients. A central mechanism of AIC is irreversible mitochondrial damage. Despite major efforts, there are currently no effective therapies able to prevent AIC.
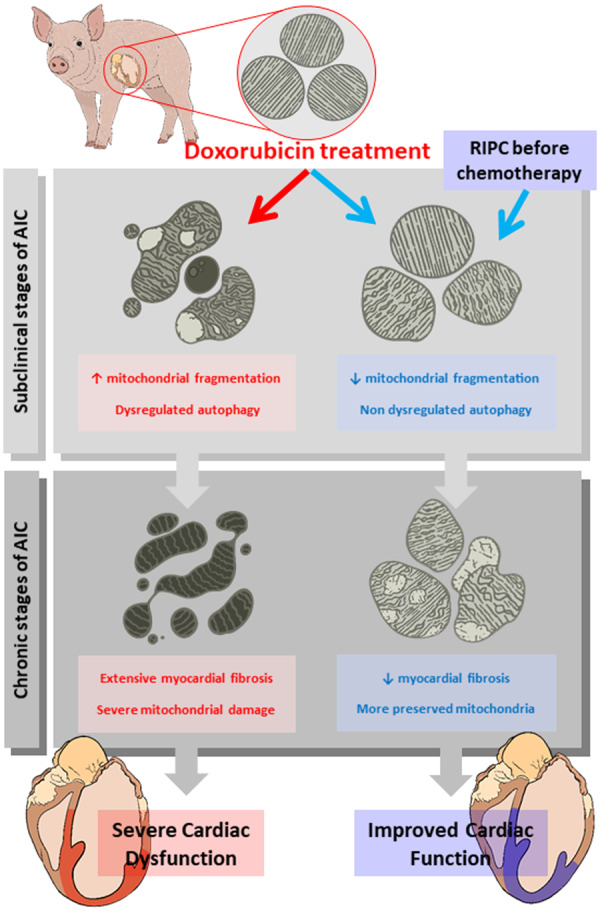
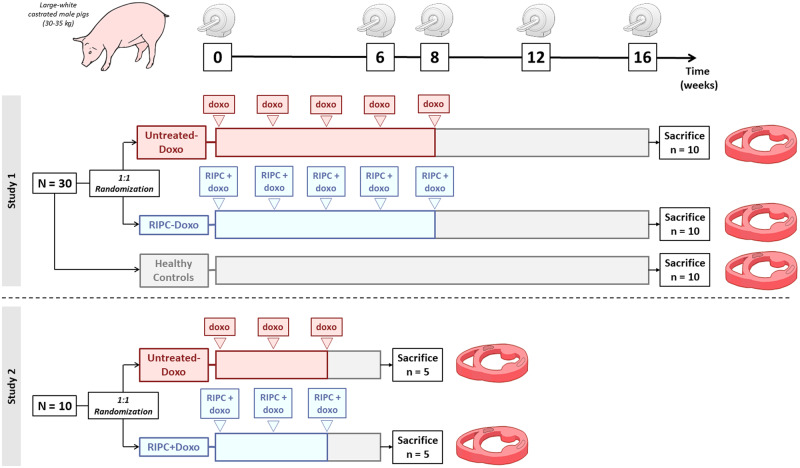
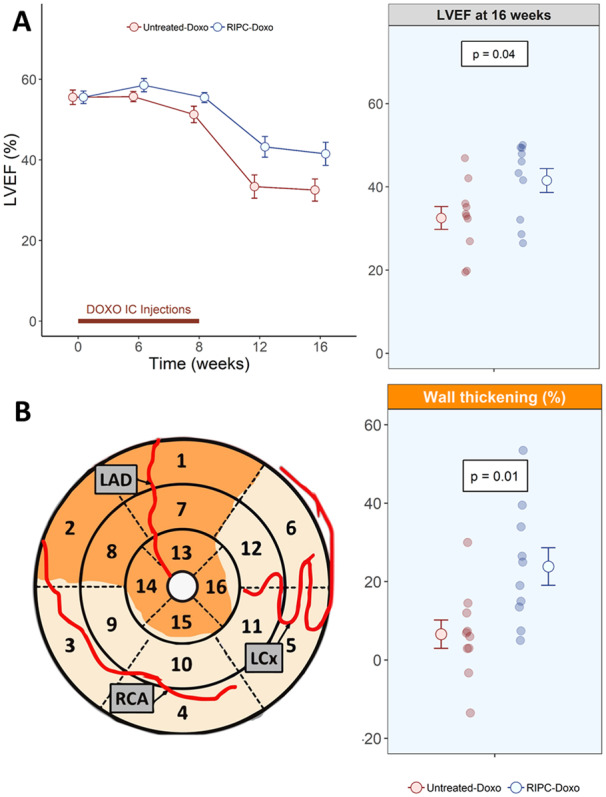
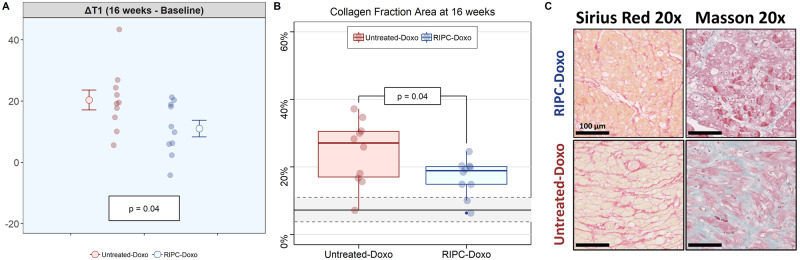
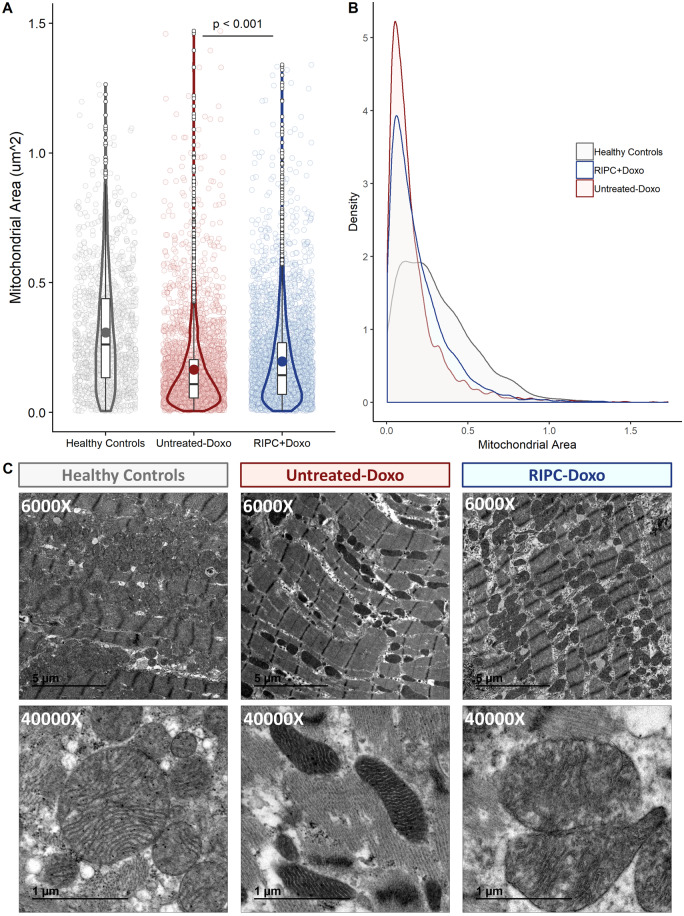
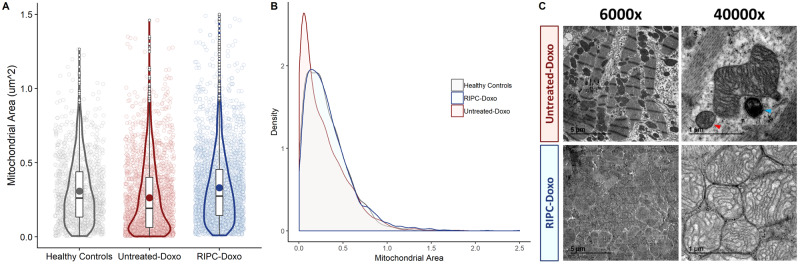
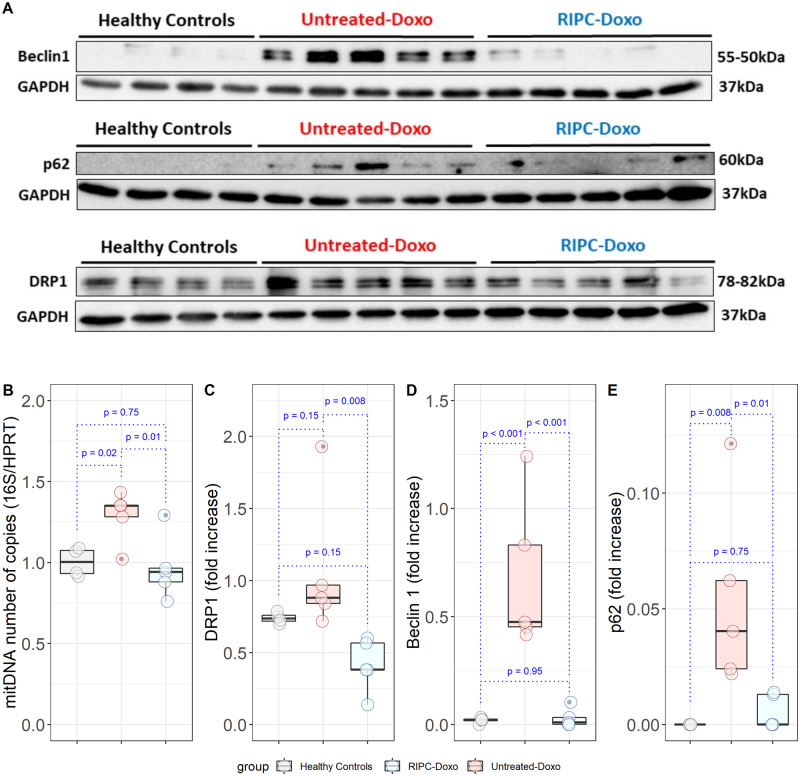
Methods and results: Forty Large-White pigs were included. In Study 1, 20 pigs were randomized 1:1 to remote ischaemic preconditioning (RIPC, 3 cycles of 5 min leg ischaemia followed by 5 min reperfusion) or no pretreatment. RIPC was performed immediately before each intracoronary doxorubicin injections (0.45 mg/kg) given at Weeks 0, 2, 4, 6, and 8. A group of 10 pigs with no exposure to doxorubicin served as healthy controls. Pigs underwent serial cardiac magnetic resonance (CMR) exams at baseline and at Weeks 6, 8, 12, and 16, being sacrifice after that. In Study 2, 10 new pigs received 3 doxorubicin injections (with/out preceding RIPC) and were sacrificed at week 6. In Study 1, left ventricular ejection fraction (LVEF) depression was blunted animals receiving RIPC before doxorubicin (RIPC-Doxo), which had a significantly higher LVEF at Week 16 than doxorubicin treated pigs that received no pretreatment (Untreated-Doxo) (41.5 ± 9.1% vs. 32.5 ± 8.7%, P = 0.04). It was mainly due to conserved regional contractile function. In Study 2, transmission electron microscopy (TEM) at Week 6 showed fragmented mitochondria with severe morphological abnormalities in Untreated-Doxo pigs, together with upregulation of fission and autophagy proteins. At the end of the 16-week Study 1 protocol, TEM revealed overt mitochondrial fragmentation with structural fragmentation in Untreated-Doxo pigs, whereas interstitial fibrosis was less severe in RIPC+Doxo pigs.
Conclusion: In a translatable large-animal model of AIC, RIPC applied immediately before each doxorubicin injection resulted in preserved cardiac contractility with significantly higher long-term LVEF and less cardiac fibrosis. RIPC prevented mitochondrial fragmentation and dysregulated autophagy from AIC early stages. RIPC is a promising intervention for testing in clinical trials in AIC.
Keywords: Anthracyclines; Cardio-oncology; Cardiotoxicity; Magnetic resonance imaging; Mitochondria; Remote conditioning.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Protection from cardiotoxicity of cancer chemotherapy: a novel target for remote ischaemic conditioning?Cardiovasc Res. 2021 Mar 21;117(4):985-986. doi: 10.1093/cvr/cvaa199. Cardiovasc Res. 2021. PMID: 32637985 No abstract available.
References
-
- Zamorano JL, Lancellotti P, Rodriguez Muñoz D, Aboyans V, Asteggiano R, Galderisi M, Habib G, Lenihan DJ, Lip GYH, Lyon AR, Lopez Fernandez T, Mohty D, Piepoli MF, Tamargo J, Torbicki A, Suter TM, Achenbach S, Agewall S, Badimon L, Barón-Esquivias G, Baumgartner H, Bax JJ, Bueno H, Carerj S, Dean V, Erol Ç, Fitzsimons D, Gaemperli O, Kirchhof P, Kolh P, et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines. Eur Heart J 2016;37:2768–2801. - PubMed
-
- López-Fernández T, López de Sá Areses E, Valbuena López SC, Dalmau González-Gallarza R, López Sendón Henchel JL, Martín García A, Santaballa Beltrán A, Montero Luis Á, García Sanz R, González Ferrer JJ, Mitroi C, Arenas M, Virizuela Echaburu JA, Marco Vera P, Barreiro-Pérez M, Mazón Ramos P, Velasco del Castillo S, Hinojar Baydes R, Zamorano JL, Pérez de Isla L, Calvo-Iglesias F, Íñiguez Romo A, Castro Fernández A, González-Caballero E, Plana Gómez JC.. Cardio-onco-hematology in clinical practice. Position paper and recommendations. Rev Esp Cardiol 2017;70:474–486. - PubMed
-
- Plana JC, Galderisi M, Barac A, Ewer MS, Ky B, Scherrer-Crosbie M, Ganame J, Sebag IA, Agler DA, Badano LP, Banchs J, Cardinale D, Carver J, Cerqueira M, Decara JM, Edvardsen T, Flamm SD, Force T, Griffin BP, Jerusalem G, Liu JE, Magalhães A, Marwick T, Sanchez LY, Sicari R, Villarraga HR, Lancellotti P.. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: a report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2014;27560:911–939. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
