

Use of General Primary Care, Specialized Primary Care, and Other Veterans Affairs Services Among High-Risk Veterans
- PMID: 32597993
- PMCID: PMC7324956
- DOI: 10.1001/jamanetworkopen.2020.8120
Use of General Primary Care, Specialized Primary Care, and Other Veterans Affairs Services Among High-Risk Veterans
Abstract
Importance: Integrated health care systems increasingly focus on improving outcomes among patients at high risk for hospitalization. Examining patterns of where patients obtain care could give health care systems insight into how to develop approaches for high-risk patient care; however, such information is rarely described.
Objective: To assess use of general and specialized primary care, medical specialty, and mental health services among patients at high risk of hospitalization in the Veterans Health Administration (VHA).
Design, setting, and participants: This national, population-based, retrospective cross-sectional study included all veterans enrolled in any type of VHA primary care service as of September 30, 2015. Data analysis was performed from April 1, 2016, to January 1, 2019.
Exposures: Risk of hospitalization and assignment to general vs specialized primary care.
Main outcome and measures: High-risk veterans were defined as those who had the 5% highest risk of near-term hospitalization based on a validated risk prediction model; all others were considered low risk. Health care service use was measured by the number of encounters in general primary care, specialized primary care, medical specialty, mental health, emergency department, and add-on intensive management services (eg, telehealth and palliative care).
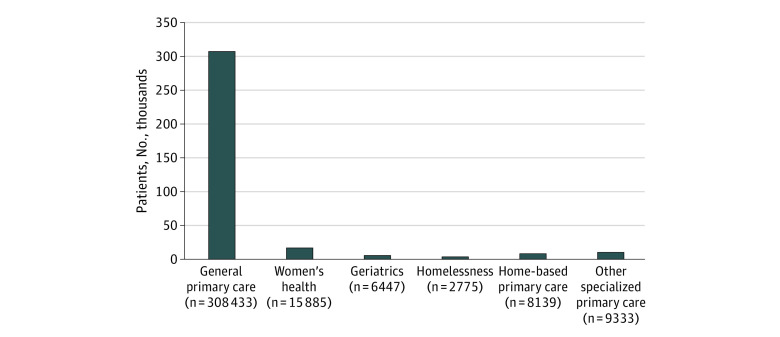
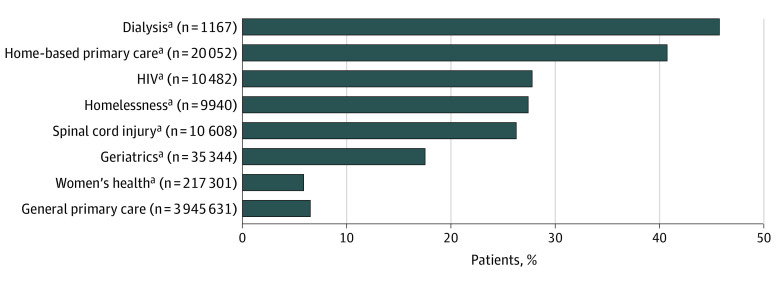
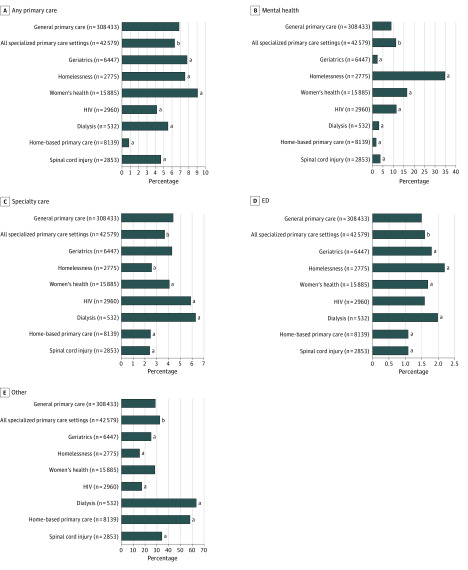
Results: The study assessed 4 309 192 veterans (mean [SD] age, 62.6 [16.0] years; 93% male). Male veterans (93%; odds ratio [OR], 1.11; 95% CI, 1.10-1.13), unmarried veterans (63%; OR, 2.30; 95% CI, 2.32-2.35), those older than 45 years (94%; 45-65 years of age: OR, 3.49 [95% CI, 3.44-3.54]; 66-75 years of age: OR, 3.04 [95% CI, 3.00-3.09]; and >75 years of age: OR, 2.42 [95% CI, 2.38-2.46]), black veterans (23%; OR, 1.63; 95% CI, 1.61-1.64), and those with medical comorbidities (asthma or chronic obstructive pulmonary disease: 33%; OR, 4.03 [95% CI, 4.00-4.06]; schizophrenia: 4%; OR, 5.14 [95% CI, 5.05-5.22]; depression: 42%; OR, 3.10 [95% CI, 3.08-3.13]; and alcohol abuse: 20%; OR, 4.54 [95% CI, 4.50-4.59]) were more likely to be high risk (n = 351 012). Most (308 433 [88%]) high-risk veterans were assigned to general primary care; the remaining 12% (42 579 of 363 561) were assigned to specialized primary care (eg, women's health and homelessness). High-risk patients assigned to general primary care had more frequent primary care visits (mean [SD], 6.9 [6.5] per year) than those assigned to specialized primary care (mean [SD], 6.3 [7.3] per year; P < .001). They also had more medical specialty care visits (mean [SD], 4.4 [5.9] vs 3.7 [5.4] per year; P < .001) and fewer mental health visits (mean [SD], 9.0 [21.6] vs 11.3 [23.9] per year; P < .001). Use of intensive supplementary outpatient services was low overall.
Conclusions and relevance: The findings suggest that, in integrated health care systems, approaches to support high-risk patient care should be embedded within general primary care and mental health care if they are to improve outcomes for high-risk patient populations.
Conflict of interest statement
Figures
Comment in
-
High-Risk Patients and Utilization of Primary Care in the US Veterans Affairs Health System.JAMA Netw Open. 2020 Jun 1;3(6):e209518. doi: 10.1001/jamanetworkopen.2020.9518. JAMA Netw Open. 2020. PMID: 32597989 No abstract available.
References
-
- Long P, Abrams M, Milstein A, et al. Effective Care for High-Need Patients: Opportunities for Improving Outcomes, Values, and Health. National Academy of Medicine; 2017. - PubMed
-
- Frandsen BR, Joynt KE, Rebitzer JB, Jha AK. Care fragmentation, quality, and costs among chronically ill patients. Am J Manag Care. 2015;21(5):355-362. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
