

Alterations in Fecal Fungal Microbiome of Patients With COVID-19 During Time of Hospitalization until Discharge
- PMID: 32598884
- PMCID: PMC7318920
- DOI: 10.1053/j.gastro.2020.06.048
Alterations in Fecal Fungal Microbiome of Patients With COVID-19 During Time of Hospitalization until Discharge
Abstract
Background & aims: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infects intestinal cells, and might affect the intestinal microbiota. We investigated changes in the fecal fungal microbiomes (mycobiome) of patients with SARS-CoV-2 infection during hospitalization and on recovery.
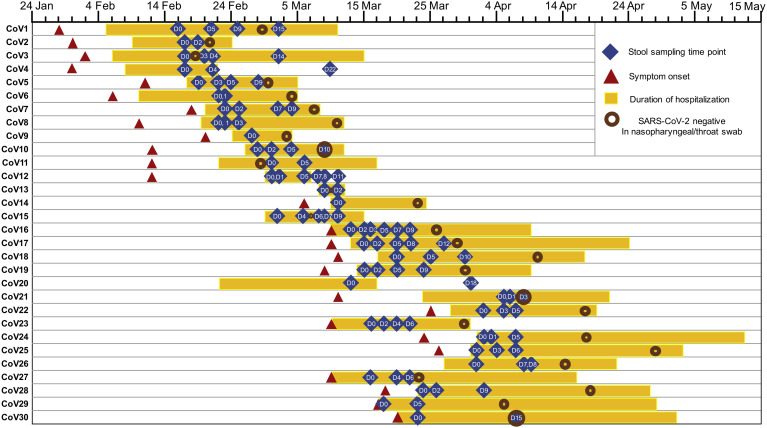
Methods: We performed deep shotgun metagenomic sequencing analysis of fecal samples from 30 patients with coronavirus disease 2019 (COVID-19) in Hong Kong, from February 5 through May 12, 2020. Fecal samples were collected 2 to 3 times per week from time of hospitalization until discharge. We compared fecal mycobiome compositions of patients with COVID-19 with those from 9 subjects with community-acquired pneumonia and 30 healthy individuals (controls). We assessed fecal mycobiome profiles throughout time of hospitalization until clearance of SARS-CoV-2 from nasopharyngeal samples.
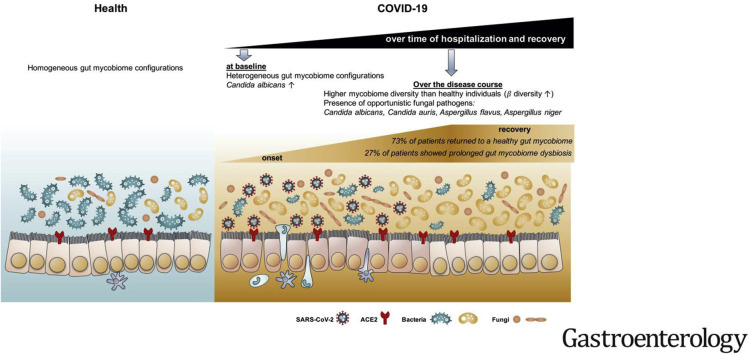
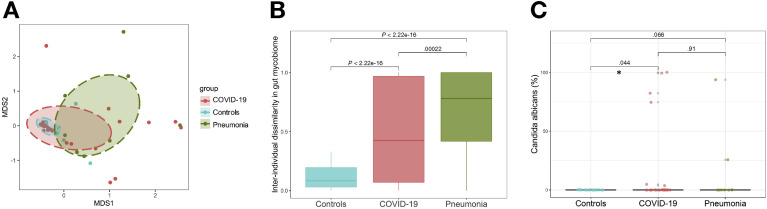
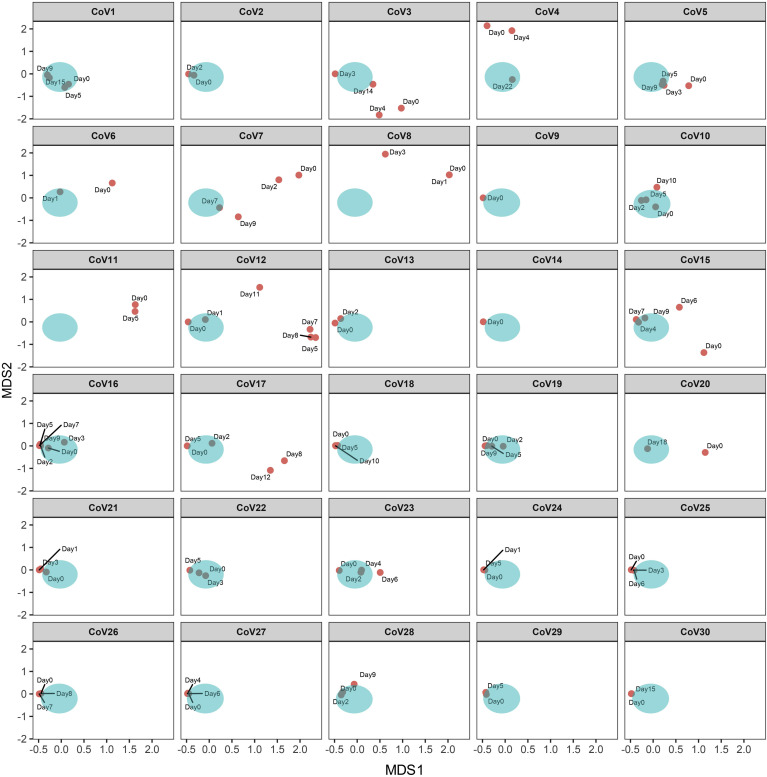
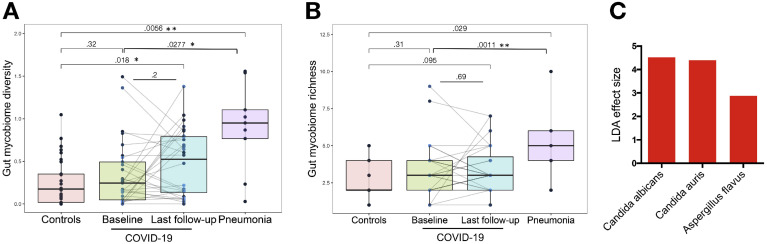
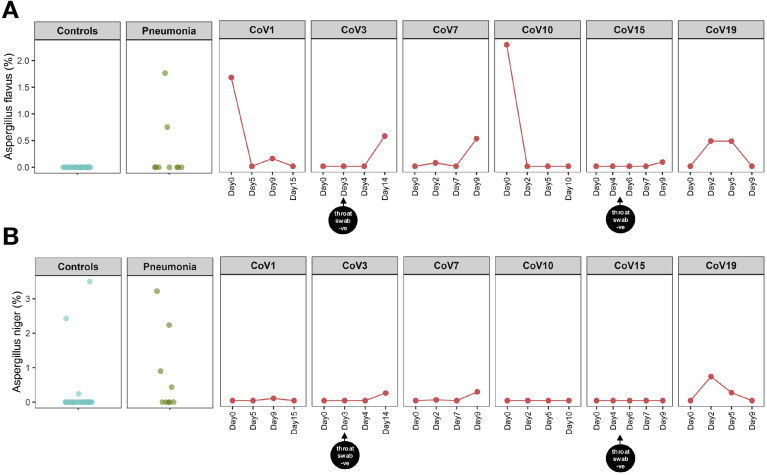
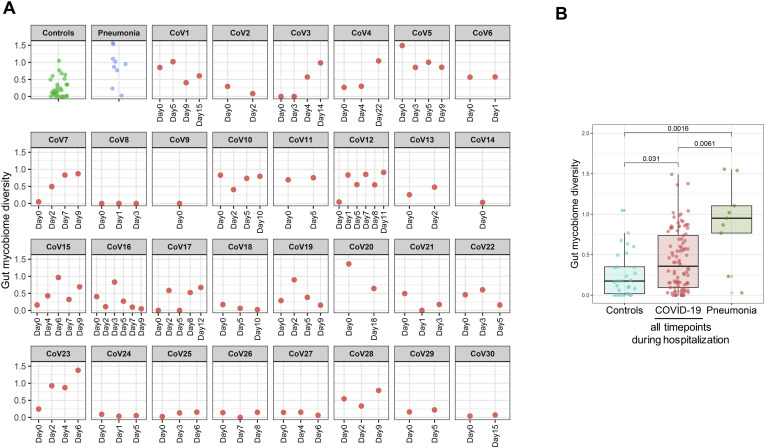
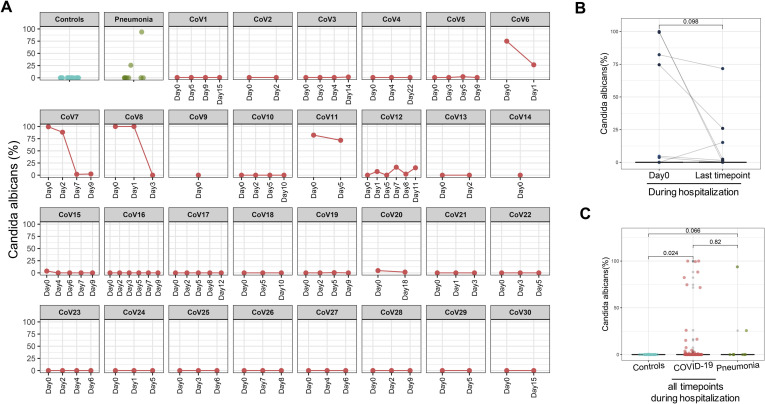
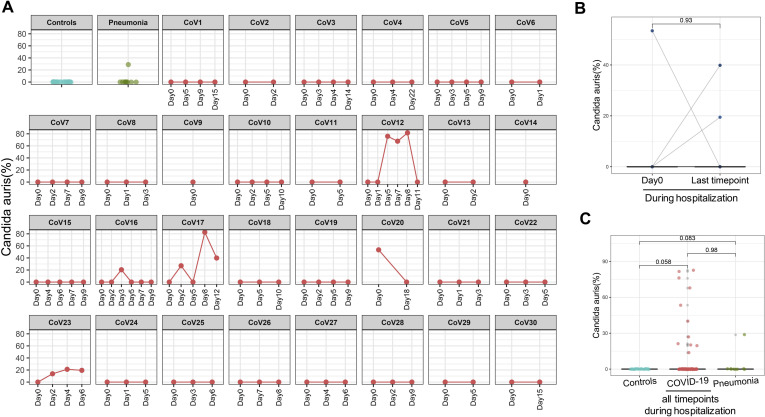
Results: Patients with COVID-19 had significant alterations in their fecal mycobiomes compared with controls, characterized by enrichment of Candia albicans and a highly heterogeneous mycobiome configuration, at time of hospitalization. Although fecal mycobiomes of 22 patients with COVID-19 did not differ significantly from those of controls during times of hospitalization, 8 of 30 patients with COVID-19 had continued significant differences in fecal mycobiome composition, through the last sample collected. The diversity of the fecal mycobiome of the last sample collected from patients with COVID-19 was 2.5-fold higher than that of controls (P < .05). Samples collected at all timepoints from patients with COVID-19 had increased proportions of opportunistic fungal pathogens, Candida albicans, Candida auris, and Aspergillus flavus compared with controls. Two respiratory-associated fungal pathogens, A. flavus and Aspergillus niger, were detected in fecal samples from a subset of patients with COVID-19, even after clearance of SARS-CoV-2 from nasopharyngeal samples and resolution of respiratory symptoms.
Conclusions: In a pilot study, we found heterogeneous configurations of the fecal mycobiome, with enrichment of fungal pathogens from the genera Candida and Aspergillus, during hospitalization of 30 patients with COVID-19 compared with controls. Unstable gut mycobiomes and prolonged dysbiosis persisted in a subset of patients with COVID-19 up to 12 days after nasopharyngeal clearance of SARS-CoV-2. Studies are needed to determine whether alterations in intestinal fungi contribute to or result from SARS-CoV-2 infection, and the effects of these changes in disease progression.
Keywords: Coronovirus; Intestine; Microbe; Yeast.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Dysbiosis in SARS-CoV-2-Infected Patients.Gastroenterology. 2021 May;160(6):2195. doi: 10.1053/j.gastro.2020.12.056. Epub 2020 Dec 30. Gastroenterology. 2021. PMID: 33387514 Free PMC article. No abstract available.
-
Reply.Gastroenterology. 2021 May;160(6):2195-2196. doi: 10.1053/j.gastro.2021.01.198. Epub 2021 Jan 21. Gastroenterology. 2021. PMID: 33484691 Free PMC article. No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
