

Prevalence and incidence of cancer related lymphedema in low and middle-income countries: a systematic review and meta-analysis
- PMID: 32600278
- PMCID: PMC7325022
- DOI: 10.1186/s12885-020-07079-7
Prevalence and incidence of cancer related lymphedema in low and middle-income countries: a systematic review and meta-analysis
Abstract
Background: Little is known about the prevalence and incidence in low and middle-income countries (LMICs) of secondary lymphedema due to cancer. The purpose of the study is to estimate the prevalence and incidence in LMICs of secondary lymphedema related to cancer and/or its treatment(s) and identify risk factors.
Method: A systematic review and meta-analysis was conducted. Medline, EMBASE and CINAHL were searched in June 2019 for peer-reviewed articles that assessed prevalence and/or incidence of cancer-related lymphedema in LMICs. Risk of bias was assessed using the Joanna Briggs Institute Critical Appraisal Checklist for Prevalence Studies. Estimates of pooled prevalence and incidence estimates were calculated with 95% confidence intervals (CI), with sub-group analyses grouping studies according to: country of origin, study design, risk of bias, setting, treatment, and lymphedema site and measurement. Heterogeneity was measured using X2 and I2, with interpretation guided by the Cochrane Handbook for Systematic Reviews.
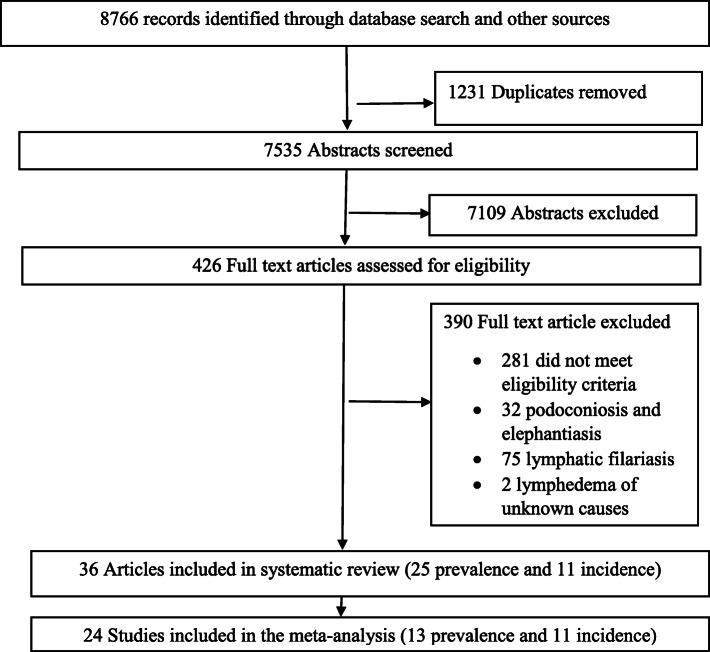
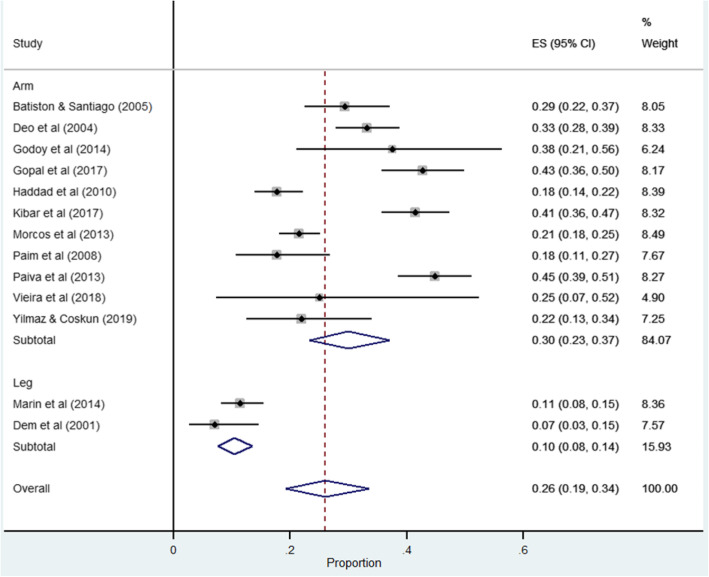
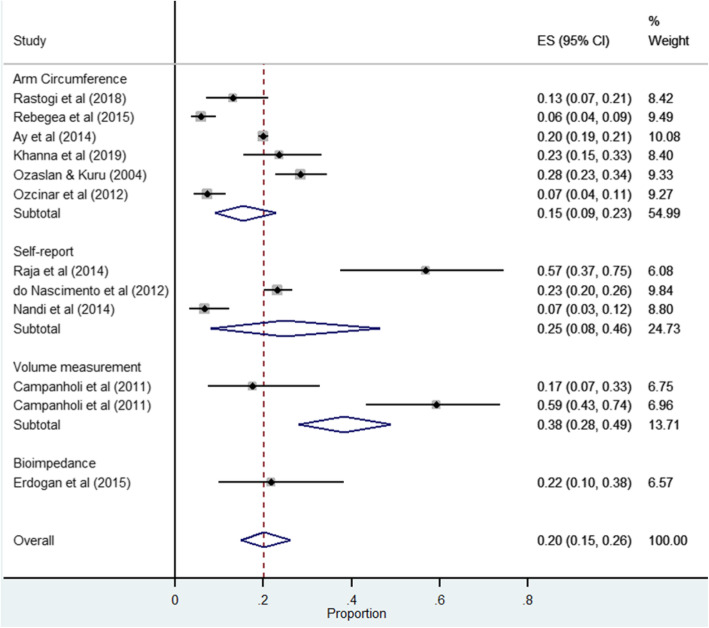
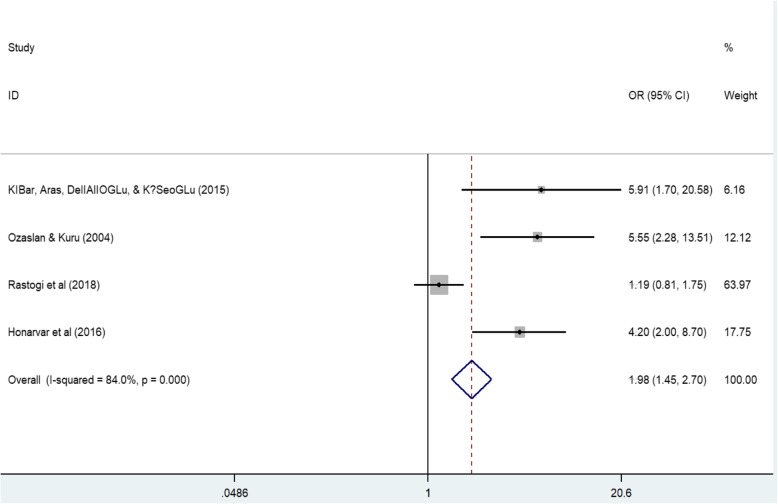
Results: Of 8766 articles, 36 were included. Most reported on arm lymphedema secondary to breast cancer treatment (n = 31), with the remainder reporting on leg lymphedema following gynecological cancer treatment (n = 5). Arm lymphedema was mostly measured by arm circumference (n = 16/31 studies), and leg lymphedema through self-report (n = 3/5 studies). Eight studies used more than one lymphedema measurement. Only two studies that measured prevalence of leg lymphedema could be included in a meta-analysis (pooled prevalence =10.0, 95% CI 7.0-13.0, I2 = 0%). The pooled prevalence of arm lymphedema was 27%, with considerable heterogeneity (95% CI 20.0-34.0, I2 = 94.69%, n = 13 studies). The pooled incidence for arm lymphedema was 21%, also with considerable heterogeneity (95% CI 15.0-26.0, I2 = 95.29%, n = 11 studies). There was evidence that higher body mass index (> 25) was associated with increased risk of arm lymphedema (OR: 1.98, 95% CI 1.45-2.70, I2 = 84.0%, P < 0.0001, n = 4 studies).
Conclusion: Better understanding the factors that contribute to variability in cancer-related arm lymphedema in LMICs is an important first step to developing targeted interventions to improve quality of life. Standardising measurement of lymphedema globally and better reporting would enable comparison within the context of information about cancer treatments and lymphedema care.
Keywords: Cancer related lymphedema; Incidence; LMICs; Lymphedema; Prevalence; Risk factor.
Conflict of interest statement
The authors declare that they have no competing interest.
Figures

References
-
- Moseley AL, Carati CJ, Piller NB. A systematic review of common conservative therapies for arm lymphoedema secondary to breast cancer treatment. Ann Oncol. 2006;18(4):639–646. - PubMed
-
- Sekyere MO. Incidence and risk factors of arm lymphedema following breast cancer treatment. American Society of Clinical Oncology. 2018.
-
- Paskett ED, Dean JA, Oliveri JM, Harrop JP. Cancer-related lymphedema risk factors, diagnosis, treatment, and impact: a review. J Clin Oncol. 2012;30(30):3726–3733. - PubMed
-
- Grada AA, Phillips TJ. Lymphedema: pathophysiology and clinical manifestations. J Am Acad Dermatol. 2017;77(6):1009–1020. - PubMed
-
- Paim CR, Lima EDR, Fu MR, Lima AP, Cassali GD. Postlymphadenectomy complications and quality of life among breast cancer patients in Brazil. Cancer Nurs. 2008;31(4):302–311. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
