

Histopathological growth patterns correlate with the immunoscore in colorectal cancer liver metastasis patients after hepatectomy
- PMID: 32601799
- PMCID: PMC11027459
- DOI: 10.1007/s00262-020-02632-6
Histopathological growth patterns correlate with the immunoscore in colorectal cancer liver metastasis patients after hepatectomy
Abstract
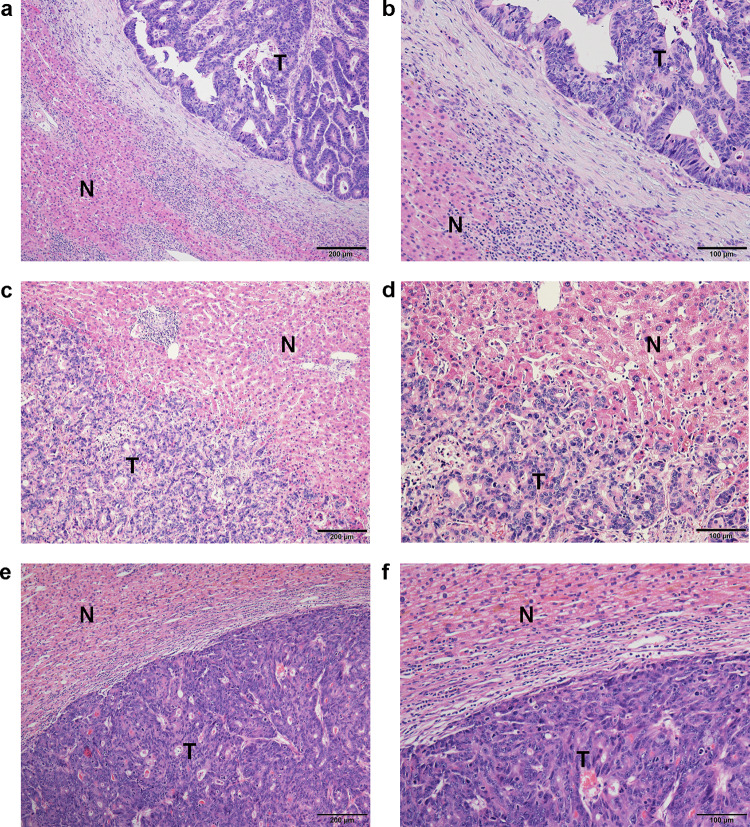
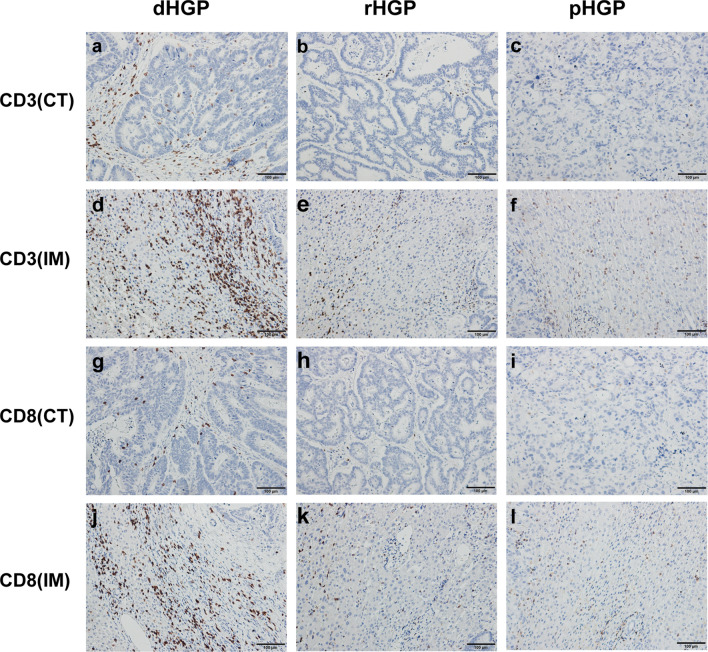
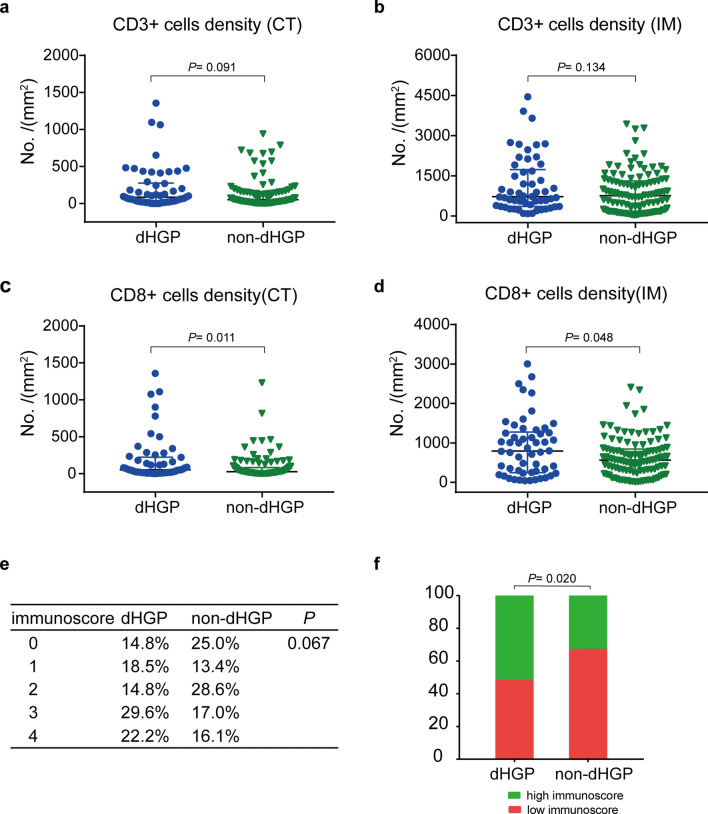
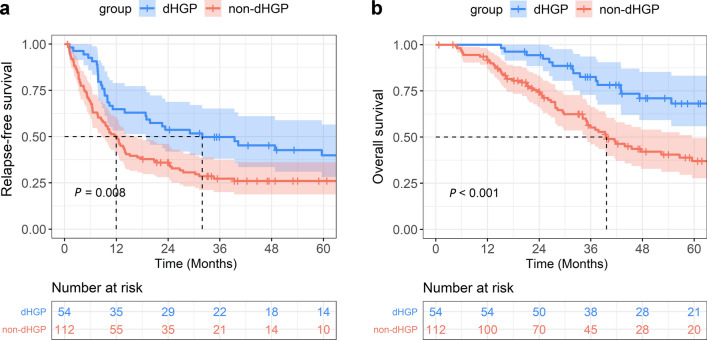
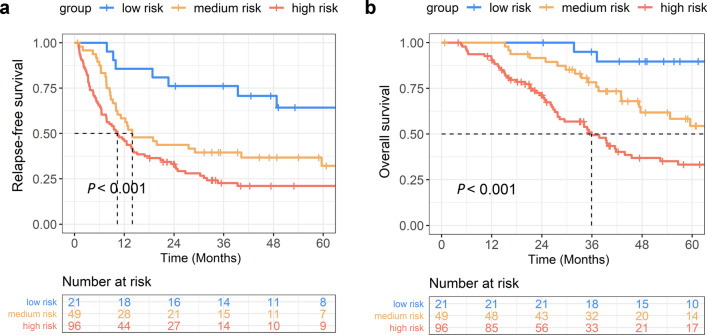
Various scoring systems have been proposed to predict the postoperative prognosis of colorectal liver metastasis (CRLM), including the clinical risk score (CRS), the immunoscore and so on. Recently, histopathological growth patterns (HGPs) have been recognized. However, the correlation between HGPs and the immunoscore, and their prognostic values in patients with CRLM after liver resection remain undetermined. In this study, HGPs were retrospectively evaluated in H&E-stained slides from 166 CRLM patients. The immunoscore was calculated according to the densities of immunostained CD3 + and CD8 + cells. A risk score combining HGPs, the immunoscore and the CRS was defined and divided patients into the low-, medium- and high-risk group. Our results showed that the densities of CD3 + and CD8 + cells were higher in the desmoplastic HGP (dHGP) group than in the non-dHGP group, and the proportion of high immunoscores was also higher in the dHGP group (51.9% vs. 33.0%, respectively, P = 0.020). Patients with the dHGP had significantly longer relapse-free survival (RFS) and overall survival (OS) than those with the non-HGP. The low-risk group showed significantly higher 2-year RFS and 5-year OS rates than the other two groups (RFS: 76.2%, 43.7% and 33.1%, respectively; P < 0.001; OS: 89.7%, 54.4% and 33.3%, respectively; P < 0.001). In conclusion, the dHGP correlates with relatively high immunoscores, predicting a favorable prognosis independent of the immunoscore and CRS. A novel risk score combining HGPs, the immunoscore and the CRS may be used for the stratification of CRLM patients' survival.
Keywords: Colorectal cancer liver metastasis; Histopathological growth patterns; Immunoscore.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures
References
-
- de Jong MC, Pulitano C, Ribero D, Strub J, Mentha G, Schulick RD, Choti MA, Aldrighetti L, Capussotti L, Pawlik TM. Rates and patterns of recurrence following curative intent surgery for colorectal liver metastasis: an international multi-institutional analysis of 1669 patients. Ann Surg. 2009;250(3):440–448. doi: 10.1097/SLA.0b013e3181b4539b. - DOI - PubMed
-
- Margonis GA, Buettner S, Andreatos N, Wagner D, Sasaki K, Barbon C, Beer A, Kamphues C, Loes IM, He J, Pawlik TM, Kaczirek K, Poultsides G, Lonning PE, Cameron JL, Mischinger HJ, Aucejo FN, Kreis ME, Wolfgang CL, Weiss MJ. Prognostic factors change over time after hepatectomy for colorectal liver metastases: a multi-institutional, international analysis of 1099 patients. Ann Surg. 2019;269(6):1129–1137. doi: 10.1097/SLA.0000000000002664. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
