

The clinical usefulness of the CTS5 in the prediction of late distant recurrence in postmenopausal women with estrogen receptor-positive early breast cancer
- PMID: 32601800
- PMCID: PMC7796868
- DOI: 10.1007/s12282-020-01130-y
The clinical usefulness of the CTS5 in the prediction of late distant recurrence in postmenopausal women with estrogen receptor-positive early breast cancer
Abstract
Background: Clinical Treatment Score post-5 years (CTS5) is a promising prognostic tool to evaluate late distant recurrence (DR) risk for breast cancer after 5-year adjuvant endocrine therapy.
Patients and methods: Among 560 postmenopausal women with pathological stage I-III estrogen receptor-positive (ER+) primary breast cancer, 383 women who had received 5-year adjuvant endocrine therapy without any recurrence at 5 years after surgery were included in this study. The CTS5 was calculated for each patient using a previously published formula, and the patients were stratified by their CTS5 values into the low-, intermediate- and high-CTS5 risk groups.
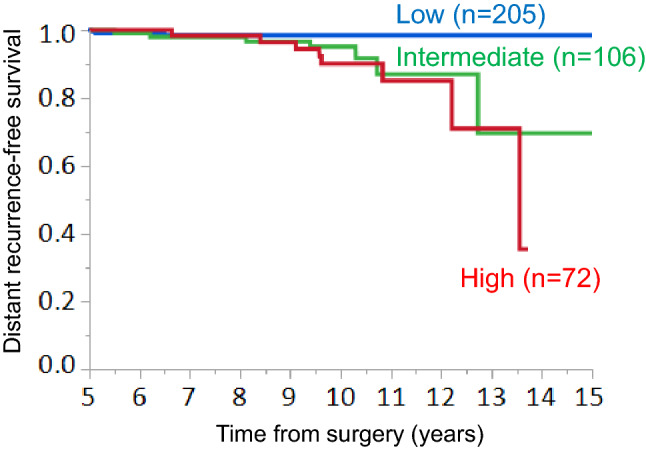
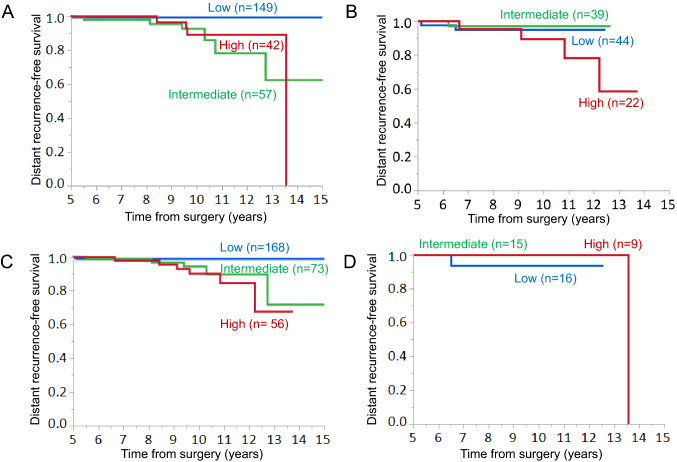
Results: According to the CTS5, 205 (53.5%), 106 (27.7%) and 72 (18.8%) patients were classified into the low-, intermediate-, and high-CTS5 risk groups, respectively. A higher ER expression level was significantly associated with the low CTS5. The increased administration of adjuvant chemotherapy was significantly associated with a high CTS5. The occurrence of DR was higher in the intermediate and high CTS5 groups than in the low CTS5 group. The DRFS in the low CTS5 risk group was significantly better than that in the intermediate- or high-risk groups. In the ER-high or HER2-negative (HER2-) group, the DRFS in the low-risk group was significantly better than that of the intermediate- or high-risk groups. However, in the low-ER or HER2-positive group, there was no significant difference in DRFS among the three risk groups.
Conclusions: In postmenopausal women with ER+ breast cancer, low CTS5 was considered to be associated with a very low risk of late DR. Thus, extended endocrine therapy may be unnecessary for patients with low CTS5 scores. Extended endocrine therapy should be offered for patients with intermediate or high CTS5 scores, especially those with high-ER and HER2- breast cancer.
Keywords: Breast cancer; CTS5; ER+; Endocrine therapy; Late distant recurrence.
Conflict of interest statement
The authors declare no conflicts of interest in association with this study.
Figures

References
-
- Matsuda T, Marugame T, Kamo K, Katanoda K, Ajiki W, Sobue T, et al. Cancer incidence and incidence rates in Japan in 2006: based on data from 15 population-based cancer registries in the monitoring of cancer incidence in Japan (MCIJ) project. Jpn J Clin Oncol. 2012;42:139–147. doi: 10.1093/jjco/hyr184. - DOI - PubMed
-
- Kurebayashi J, Miyoshi Y, Ishikawa T, Saji S, Sugie T, Suzuki T, et al. Clinicopathological characteristics of breast cancer and trends in the management of breast cancer patients in Japan: based on the Breast Cancer Registry of the Japanese Breast Cancer Society between 2004 and 2011. Breast Cancer. 2015;22:235–244. doi: 10.1007/s12282-015-0599-6. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
