

Parkinson disease clinical subtypes: key features & clinical milestones
- PMID: 32602253
- PMCID: PMC7448190
- DOI: 10.1002/acn3.51102
Parkinson disease clinical subtypes: key features & clinical milestones
Abstract
Objectives: Based on multi-domain classification of Parkinson disease (PD) subtypes, we sought to determine the key features that best differentiate subtypes and the utility of PD subtypes to predict clinical milestones.
Methods: Prospective cohort of 162 PD participants with ongoing, longitudinal follow-up. Latent class analysis (LCA) delineated subtypes based on score patterns across baseline motor, cognitive, and psychiatric measures. Discriminant analyses identified key features that distinguish subtypes at baseline. Cox regression models tested PD subtype differences in longitudinal conversion to clinical milestones, including deep brain stimulation (DBS), dementia, and mortality.
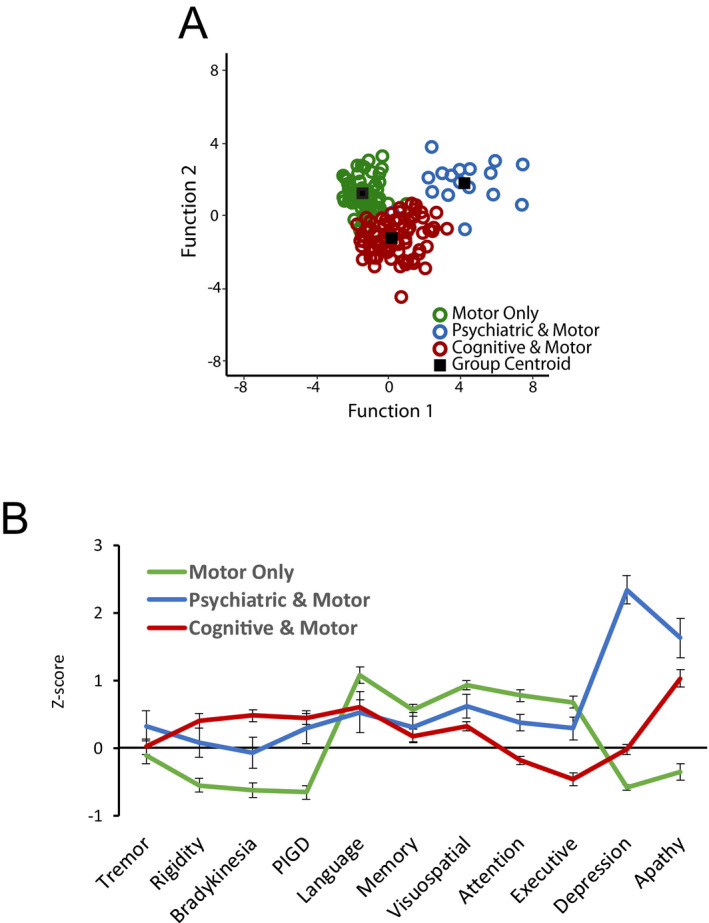
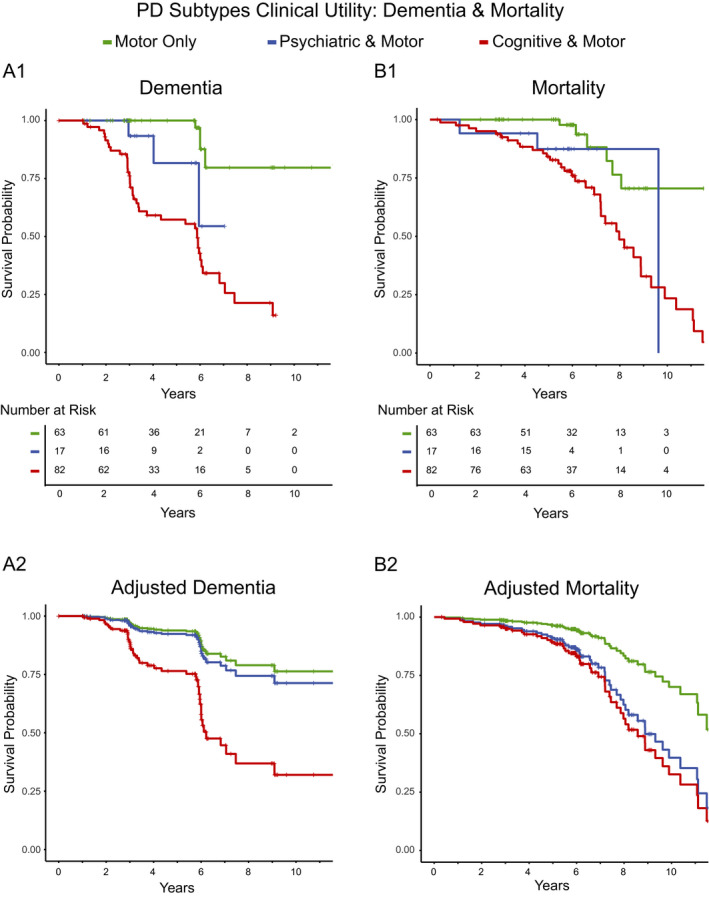
Results: LCA identified distinct subtypes: "motor only" (N = 63) characterized by primary motor deficits; "psychiatric & motor" (N = 17) characterized by prominent psychiatric symptoms and moderate motor deficits; "cognitive & motor" (N = 82) characterized by impaired cognition and moderate motor deficits. Depression, executive function, and apathy best discriminated subtypes. Since enrollment, 22 had DBS, 48 developed dementia, and 46 have died. Although there were no subtype differences in rate of DBS, dementia occurred at a higher rate in the "cognitive & motor" subtype. Surprisingly, mortality risk was similarly elevated for both "cognitive & motor" and "psychiatric & motor" subtypes compared to the "motor only" subtype (relative risk = 3.15, 2.60).
Interpretation: Psychiatric and cognitive features, rather than motor deficits, distinguish clinical PD subtypes and predict greater risk of subsequent dementia and mortality. These results emphasize the value of multi-domain assessments to better characterize clinical variability in PD. Further, differences in dementia and mortality rates demonstrate the prognostic utility of PD subtypes.
© 2020 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
Dr. Campbell receives salary and research support from the NIH, American Parkinson Disease Association (APDA) Advanced Research Center for PD at WUSTL; Greater St. Louis Chapter of the APDA; McDonnell Center for Systems Neuroscience; Department of Radiology at WUSTL. She also received honoraria from the Department of Veterans Affairs and the Parkinson Foundation. Dr. Myers receives salary and research support from NIH. Ms. Weigand receives salary and research support from NSF. Dr. Foster receives salary and research support from the NIH and American Parkinson Disease Association (APDA) Advanced Research Center for PD at WUSTL; Greater St. Louis Chapter of the APDA. Dr. Cairns receives salary and research support from NIH and the University of Exeter. Dr. Jackson receives salary and research support from NIH and Washington University in St. Louis. Dr. Lessov‐Schlaggar receives salary and research support from NIH. Dr. Perlmutter receives salary and research support from NIH, Washington University in St. Louis, American Parkinson Disease Association (APDA), Greater St. Louis Chapter of the APDA, McDonnell Center for Higher Brain Function, Barnes‐Jewish Hospital Foundation, Huntington’s Disease Society of America, CHDI, MJ Fox Foundation, Fixel Foundation, Oertli Foundation, Riney Foundation and Washington University CTSA/ICTS. He also received honoraria from the American Academy of Neurology, University of Rochester, Parkinson Disease Foundation, St Louis Univ., Harvard, Univ. Michigan, Stanford, CHDI, Huntington Study Group.
Figures
References
-
- Sauerbier A, Jenner P, Todorova A, Chaudhuri KR. Non motor subtypes and Parkinson's disease. Parkinson Relat Disord 2016;22(Suppl 1):S41–S46. - PubMed
-
- Fereshtehnejad SM, Zeighami Y, Dagher A, Postuma RB. Clinical criteria for subtyping Parkinson's disease: biomarkers and longitudinal progression. Brain 2017;140:1959–1976. - PubMed
-
- Marras C, Chaudhuri KR. Nonmotor features of Parkinson's disease subtypes. Mov Disord 2016;31:1095–1102. - PubMed
Publication types
MeSH terms
Grants and funding
- NS41509/NS/NINDS NIH HHS/United States
- UL1 RR024992/RR/NCRR NIH HHS/United States
- R01 NS075321/NS/NINDS NIH HHS/United States
- R01 NS041509/NS/NINDS NIH HHS/United States
- R01 NS058714/NS/NINDS NIH HHS/United States
- UL1 TR002345/TR/NCATS NIH HHS/United States
- RF1 NS075321/NS/NINDS NIH HHS/United States
- NS075321/NS/NINDS NIH HHS/United States
- K08 NS048924/NS/NINDS NIH HHS/United States
- NS058714/NS/NINDS NIH HHS/United States
- NS097437/NS/NINDS NIH HHS/United States
- NS48924/NS/NINDS NIH HHS/United States
- P30 NS048056/NS/NINDS NIH HHS/United States
- R01 NS097437/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
