

Mechanism of Action of OnabotulinumtoxinA in Chronic Migraine: A Narrative Review
- PMID: 32602955
- PMCID: PMC7496564
- DOI: 10.1111/head.13849
Mechanism of Action of OnabotulinumtoxinA in Chronic Migraine: A Narrative Review
Abstract
Objective: To review the literature on the mechanism of action of onabotulinumtoxinA in chronic migraine.
Background: OnabotulinumtoxinA is a chronic migraine preventive treatment that significantly reduces headache frequency. The traditional mechanism described for onabotulinumtoxinA - reducing muscle contractions - is insufficient to explain its efficacy in migraine, which is primarily a sensory neurological disease.
Methods: A narrative literature review on the mechanism of action of onabotulinumtoxinA in chronic migraine.
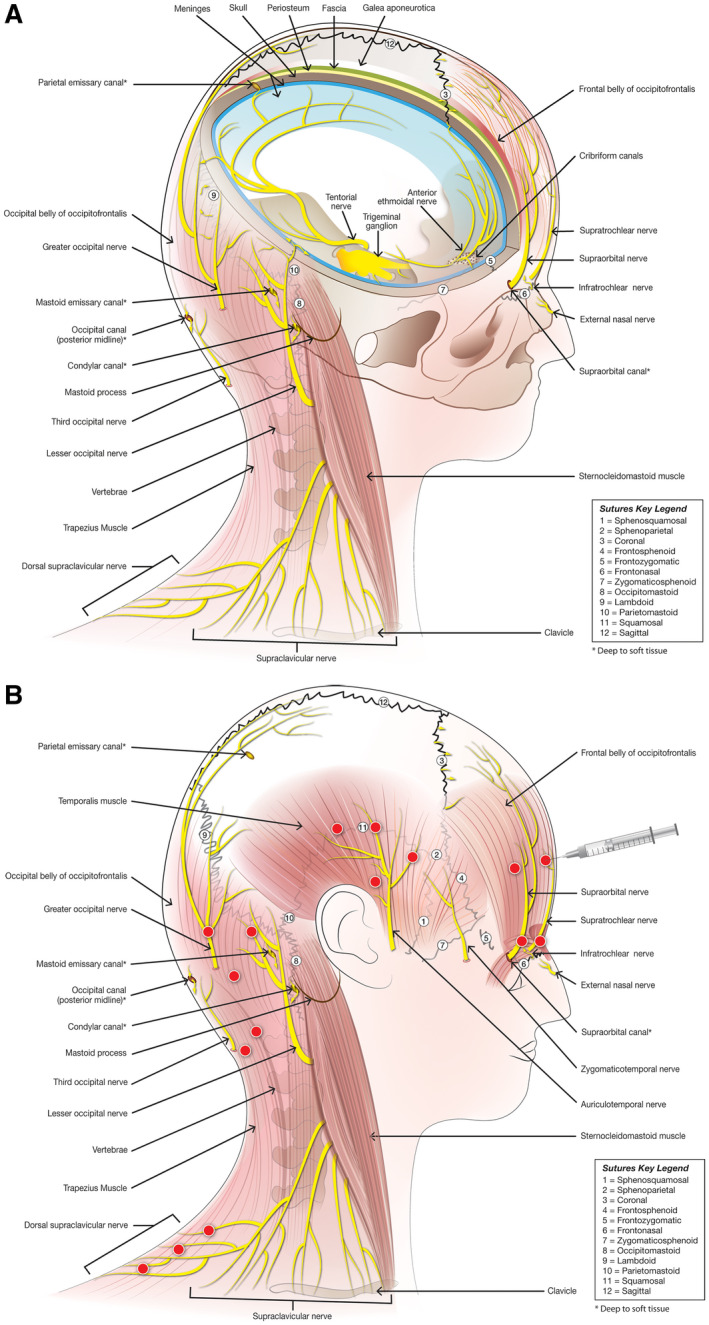
Results: Following injection into tissues, onabotulinumtoxinA inhibits soluble N-ethylmaleimide-sensitive fusion attachment protein receptor (SNARE)-mediated vesicle trafficking by cleaving one of its essential proteins, soluble N-ethylmaleimide-sensitive fusion attachment protein (SNAP-25), which occurs in both motor and sensory nerves. OnabotulinumtoxinA inhibits regulated exocytosis of motor and sensory neurochemicals and proteins, as well as membrane insertion of peripheral receptors that convey pain from the periphery to the brain, because both processes are SNARE dependent. OnabotulinumtoxinA can decrease exocytosis of pro-inflammatory and excitatory neurotransmitters and neuropeptides such as substance P, calcitonin gene-related peptide, and glutamate from primary afferent fibers that transmit nociceptive pain and participate in the development of peripheral and central sensitization. OnabotulinumtoxinA also decreases the insertion of pain-sensitive ion channels such as transient receptor potential cation channel subfamily V member 1 (TRPV1) into the membranes of nociceptive neurons; this is likely enhanced in the sensitized neuron. For chronic migraine prevention, onabotulinumtoxinA is injected into 31-39 sites in 7 muscles of the head and neck. Sensory nerve endings of neurons whose cell bodies are located in trigeminal and cervical ganglia are distributed throughout the injected muscles, and are overactive in people with migraine. Through inhibition of these sensory nerve endings, onabotulinumtoxinA reduces the number of pain signals that reach the brain and consequently prevents activation and sensitization of central neurons postulated to be involved in migraine chronification.
Conclusion: OnabotulinumtoxinA likely acts via sensory mechanisms to treat chronic migraine.
Keywords: botulinum; headache; migraine; trigeminal system.
© 2020 The Authors. Headache: The Journal of Head and Face Pain published by Wiley Periodicals LLC on behalf of American Headache Society.
Figures

References
-
- Scott AB. Botulinum toxin injection into extraocular muscles as an alternative to strabismus surgery. Ophthalmology. 1980;87:1044‐1049. - PubMed
-
- Scott AB, Kennedy RA, Stubbs HA. Botulinum A toxin injection as a treatment for blepharospasm. Arch Ophthalmol. 1985;103:347‐350. - PubMed
-
- Simpson DM, Hallett M, Ashman EJ, et al. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2016;86:1818‐1826. - PMC - PubMed
-
- Tsui JK, Eisen A, Mak E, Carruthers J, Scott A, Calne DB. A pilot study on the use of botulinum toxin in spasmodic torticollis. Can J Neurol Sci. 1985;12:314‐316. - PubMed
-
- Tsui JK, Eisen A, Stoessl AJ, Calne S, Calne DB. Double‐blind study of botulinum toxin in spasmodic torticollis. Lancet. 1986;2:245‐247. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
