

Everolimus improves the efficacy of dasatinib in PDGFRα-driven glioma
- PMID: 32603316
- PMCID: PMC7524471
- DOI: 10.1172/JCI133310
Everolimus improves the efficacy of dasatinib in PDGFRα-driven glioma
Abstract
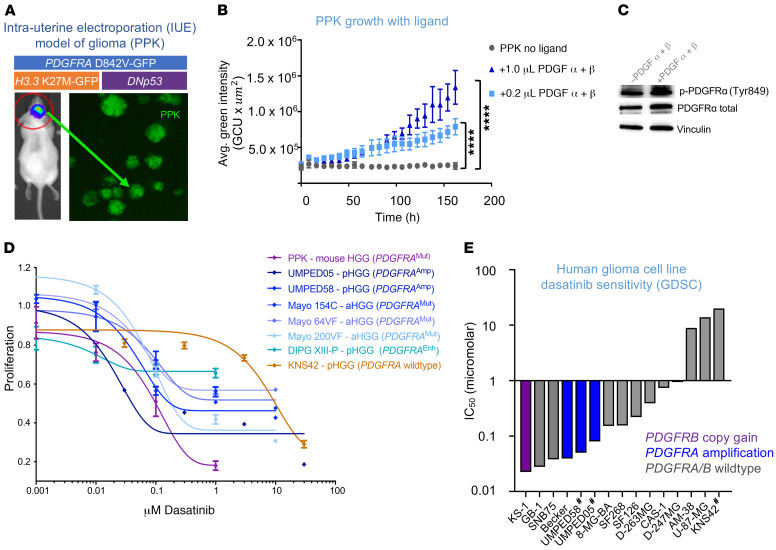
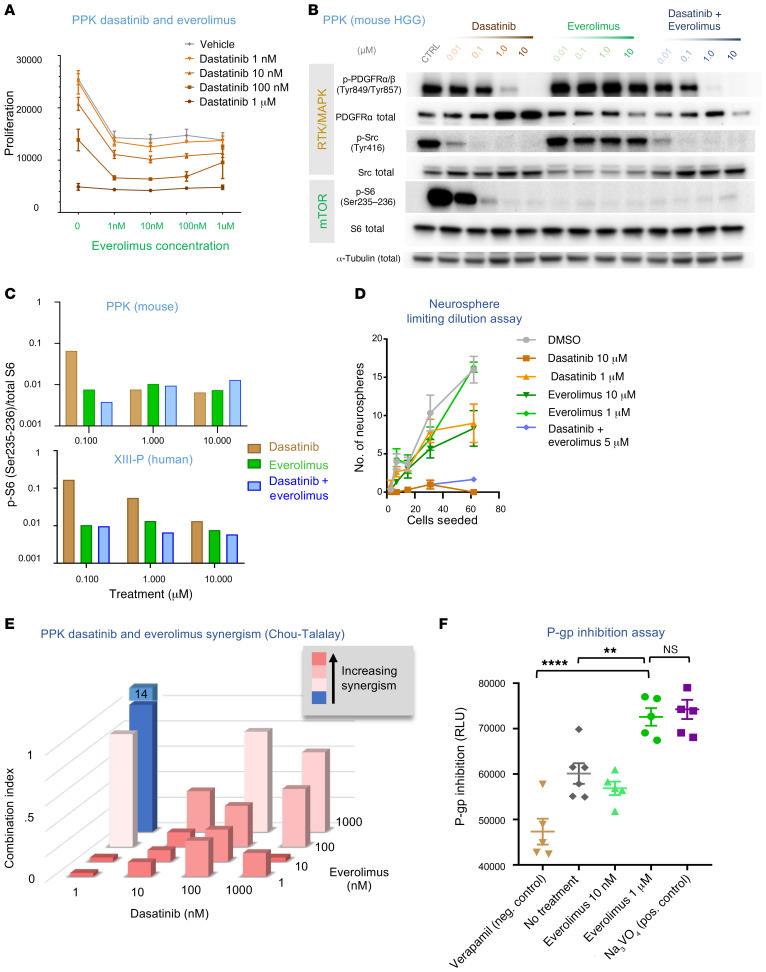
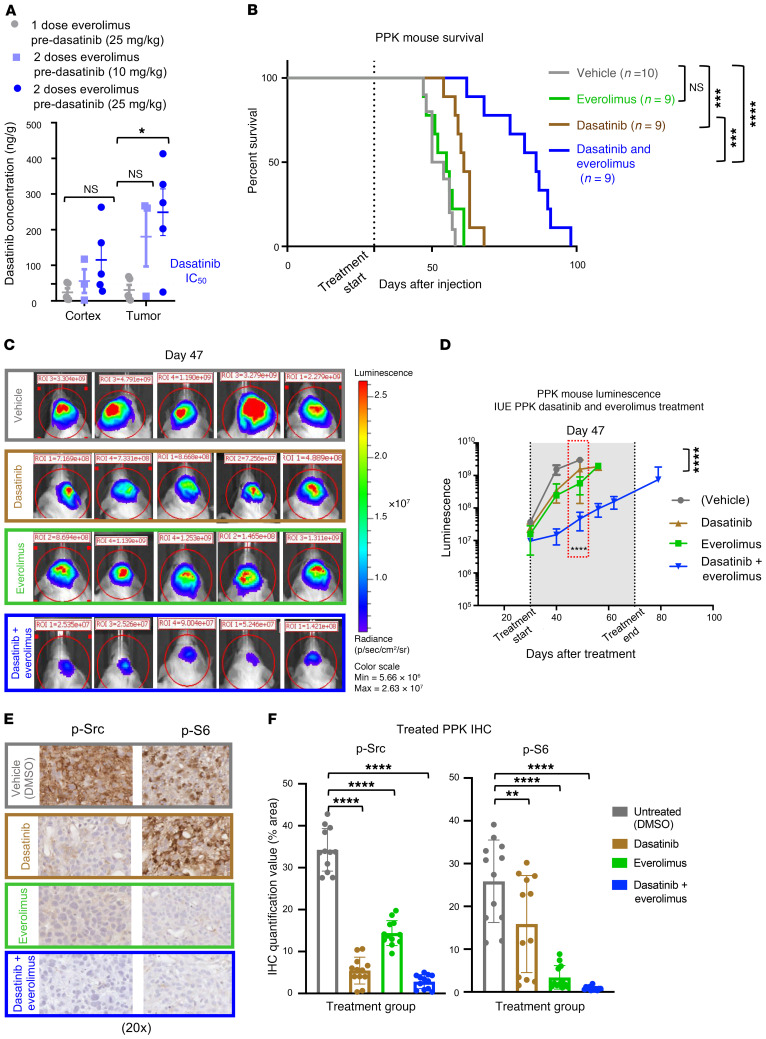
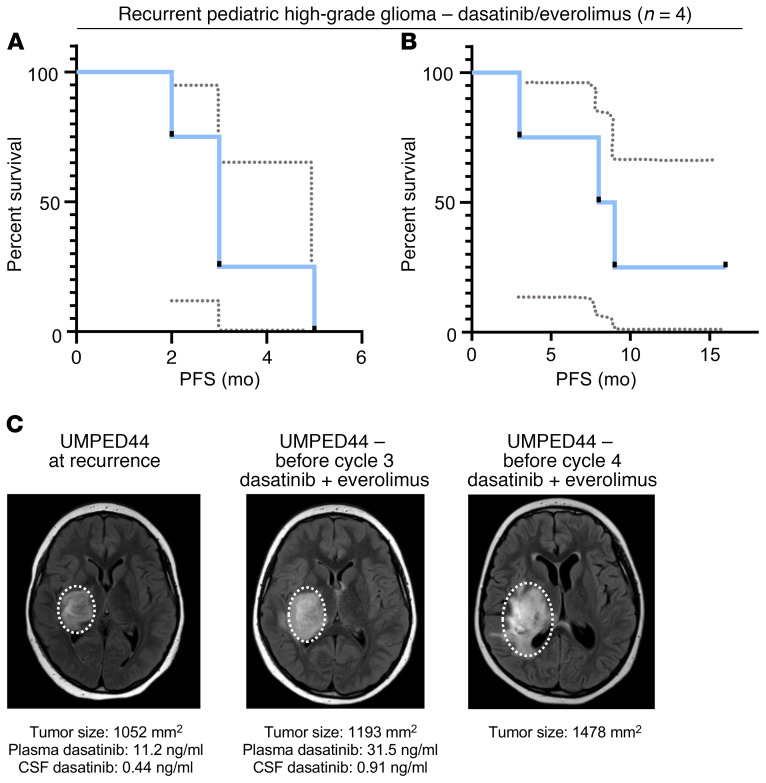
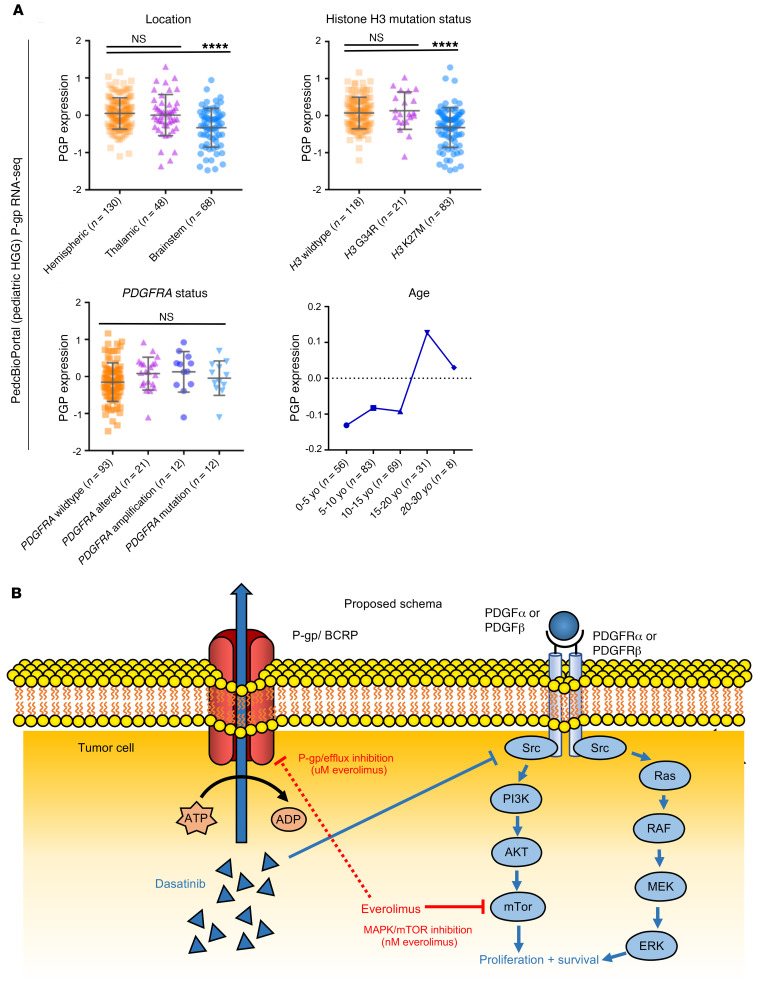
Pediatric and adult high-grade gliomas (HGGs) frequently harbor PDGFRA alterations. We hypothesized that cotreatment with everolimus may improve the efficacy of dasatinib in PDGFRα-driven glioma through combinatorial synergism and increased tumor accumulation of dasatinib. We performed dose-response, synergism, P-glycoprotein inhibition, and pharmacokinetic studies in in vitro and in vivo human and mouse models of HGG. Six patients with recurrent PDGFRα-driven glioma were treated with dasatinib and everolimus. We found that dasatinib effectively inhibited the proliferation of mouse and human primary HGG cells with a variety of PDGFRA alterations. Dasatinib exhibited synergy with everolimus in the treatment of HGG cells at low nanomolar concentrations of both agents, with a reduction in mTOR signaling that persisted after dasatinib treatment alone. Prolonged exposure to everolimus significantly improved the CNS retention of dasatinib and extended the survival of PPK tumor-bearing mice (mutant TP53, mutant PDGFRA, H3K27M). Six pediatric patients with glioma tolerated this combination without significant adverse events, and 4 patients with recurrent disease (n = 4) had a median overall survival of 8.5 months. Our results show that the efficacy of dasatinib treatment of PDGFRα-driven HGG was enhanced with everolimus and suggest a promising route for improving targeted therapy for this patient population.
Keywords: Brain cancer; Molecular biology; Oncology; Pharmacology.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
