

Rehospitalization for pneumonia after first pneumonia admission: Incidence and predictors in a population-based cohort study
- PMID: 32603334
- PMCID: PMC7326167
- DOI: 10.1371/journal.pone.0235468
Rehospitalization for pneumonia after first pneumonia admission: Incidence and predictors in a population-based cohort study
Abstract
Background and objectives: Hospital readmissions are a frequent complication of pneumonia. Most data regarding readmissions are obtained from the United States, whereas few data are available from the European healthcare utilization (HCU) systems. In a large cohort of Italian patients with a previous hospitalization for pneumonia, our aim was to evaluate the incidence and predictors of early readmissions due to pneumonia.
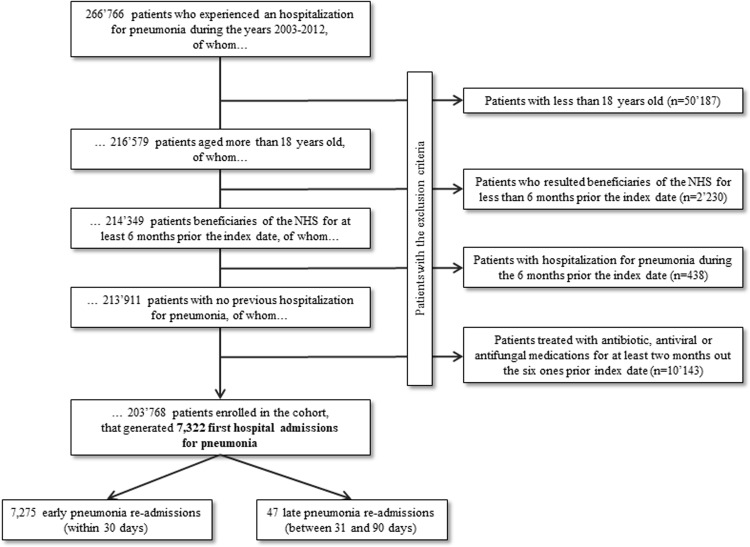
Methods: This is a observational retrospective, population based, cohort study. Data were retrieved from the HCU databases of the Italian Lombardy region. 203,768 patients were hospitalized for pneumonia between 2003 and 2012. The outcome was the first rehospitalization for pneumonia. The patients were followed up after the index hospital admission to estimate the hazard ratio, and relative 95% confidence interval, of the outcome associated with the risk factors that we had identified.
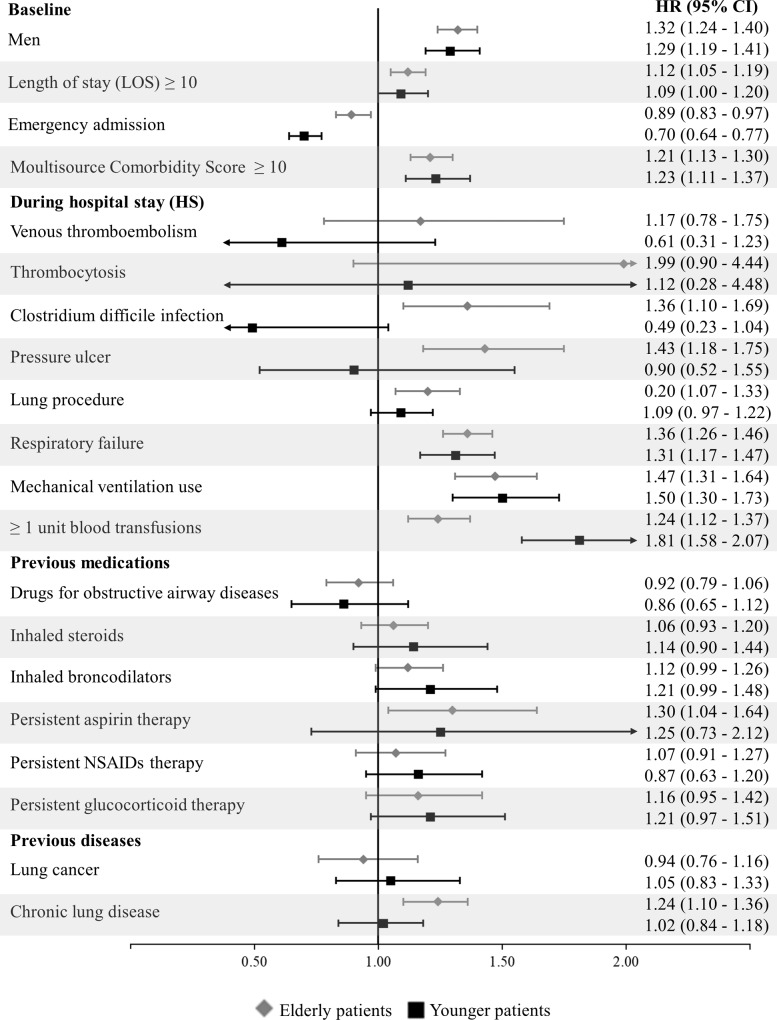
Results: 7,275 patients (3.6%) had an early pneumonia readmission. Male gender, age ≥70 years, length of stay of the first admission and a higher burden of comorbidities were significantly associated with the outcome. Chronic use of antidepressants, antiarrhythmics, glucocorticoids and drugs for obstructive airway diseases were also more frequently prescribed in patients requiring rehospitalization. Previous use of inhaled broncodilators, including both beta2-agonists and anticholinergics, but not inhaled steroids, were associated with an increased risk of hospital readmission.
Conclusions: Frail elderly patients with multiple comorbidities and complex drug regimens were at higher risk of early rehospitalization and, thus, may require closer follow-up and prevention strategies.
Conflict of interest statement
The authors have read the journal's policy and the authors of this manuscript have the following competing interests: G.C. received research support from the European Community (EC), the Italian Medicines Agency (AIFA), and the Italian Ministry of Education, Universities and Research (MIUR). He took part in a variety of projects that were funded by pharmaceutical companies (Novartis, GSK, Roche, AMGEN and BMS). He also received honoraria as a member of the Advisory Board of Roche. No other potential conflicts of interest were declared. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
