

What Is the Survivorship After Hip Arthroscopy for Femoroacetabular Impingement? A Large-database Study
- PMID: 32604156
- PMCID: PMC7491898
- DOI: 10.1097/CORR.0000000000001370
What Is the Survivorship After Hip Arthroscopy for Femoroacetabular Impingement? A Large-database Study
Abstract
Background: Patients with femoroacetabular impingement (FAI) may experience lasting clinical improvement after hip arthroscopy; however, some patients will still eventually undergo early conversion to THA due to unresolved symptoms and progression of arthritis. However, the risk of this has been only incompletely characterized in prior studies.
Questions/purposes: Using a large healthcare claims database over a 5-year period (2011-2016), we asked: (1) What is the survivorship free from THA after arthroscopic osteoplasty performed for FAI? (2) What identifiable demographic factors and patient characteristics are associated with early conversion to THA after hip arthroscopy performed for FAI?
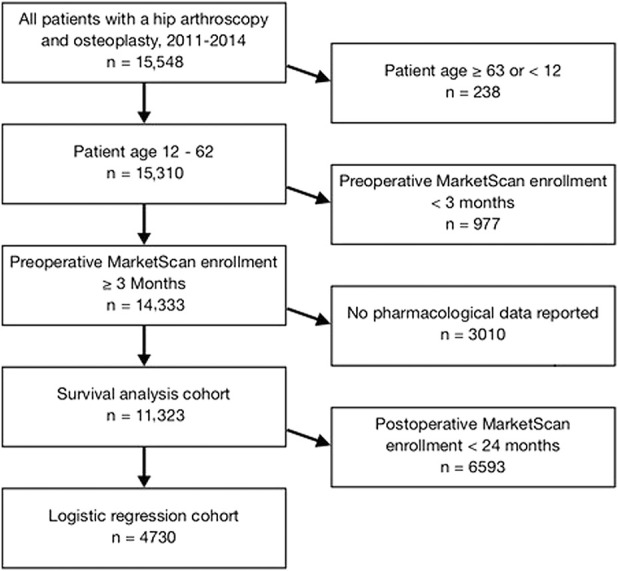
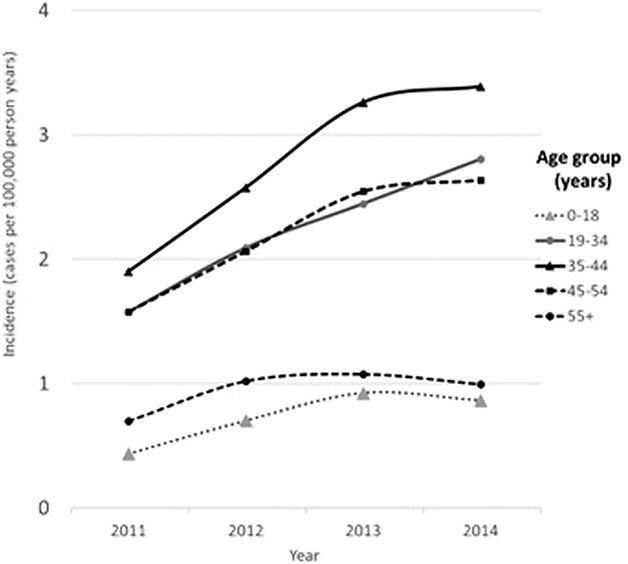
Methods: We included all patients who underwent hip arthroscopy for FAI, between the ages of 12 years and 63 years, with 3 months of claims data before hip arthroscopy and minimum 2-year follow-up. A total of 4730 hip arthroscopy patients from 2011 to 2014 were retrieved from a US commercial claims database. Hip arthroscopy incidence doubled over time from 1.2 to 2.1 persons per 100,000. Temporal trends, patient demographics, diagnoses at time of arthroscopy, and patient comorbidities were retrieved and logistic regression performed. Survivorship analysis on 11,323 patients (lifting the 2-year follow-up requirement) was also performed to identify independent variables associated with early risk of conversion to THA.
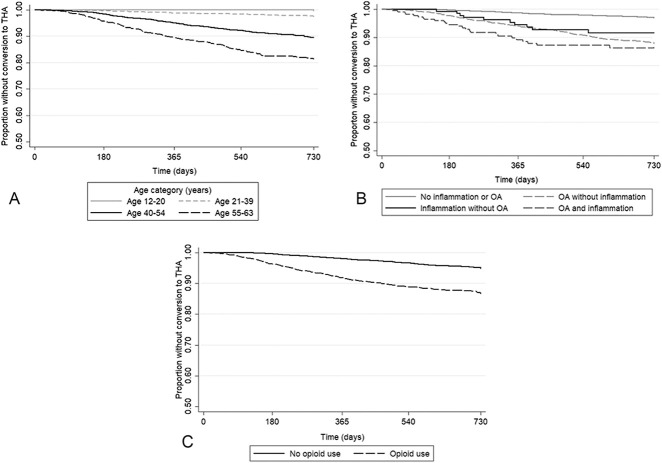
Results: In patients undergoing hip arthroscopy for FAI, the overall proportion of conversion to THA within 2 years after hip arthroscopy was 7% (338 of 4730). After controlling for confounding variables such as sex, obesity, and depression, we found the following were independently associated with increased odds of conversion to THA: older age (odds ratio 1.08 [95% CI 1.01 to 1.10]; p < 0.001), osteoarthritis (OR 2.91 [95% CI 2.27 to 3.77]; p < 0.001), joint inflammation (OR 1.89 [95% CI 1.16 to 3.09]; p = 0.01), and a history of opioid use (OR 2.17 [95% CI 1.69 to 2.79]; p < 0.001). Survivorship analysis similarly revealed that older age (hazard ratio 1.08 [95% CI 1.07 to 1.09]; p < 0.001), osteoarthritis (HR 2.53 [95% CI 2.13 to 3.01]; p < 0.001), joint inflammation (HR 1.53 [95% CI 1.10 to 2.11]; p = 0.01), a history of opioid use (HR 2.02 [95% CI 1.71 to 2.38]; p < 0.001), and smoking (HR 1.55 [95% CI 1.14 to 2.11]; p = 0.005), were independently associated with increased odds of conversion to THA within 2 years after hip arthroscopy for FAI.
Conclusions: Although the findings of this study are limited and should not be taken in isolation, patients with FAI who are older, carry diagnoses of inflammatory or degenerative articular disease, or who use opioids or smoke should be counseled about a potentially increased risk of undergoing early conversion to THA after hip arthroscopy. Future studies to further examine the effect of these diagnoses in prospectively collected cohorts, incorporating radiographic and patient-reported outcome measures, are needed.
Level of evidence: Level III, prognostic study.
Conflict of interest statement
Each author certifies that neither he or she, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR Insights®: What Is the Survivorship After Hip Arthroscopy for Femoroacetabular Impingement? A Large-database Study.Clin Orthop Relat Res. 2020 Oct;478(10):2274-2276. doi: 10.1097/CORR.0000000000001442. Clin Orthop Relat Res. 2020. PMID: 32769544 Free PMC article. No abstract available.
Similar articles
-
Good Outcome Scores and Low Conversion Rate to THA 10 Years After Hip Arthroscopy for the Treatment of Femoroacetabular Impingement.Clin Orthop Relat Res. 2021 Oct 1;479(10):2256-2264. doi: 10.1097/CORR.0000000000001778. Clin Orthop Relat Res. 2021. PMID: 33929975 Free PMC article.
-
Association Between Chondrolabral Junction Breakdown and Conversion to Total Hip Arthroplasty After Hip Arthroscopy for Symptomatic Labral Tears: Minimum 8-Year Follow-up.Am J Sports Med. 2024 Apr;52(5):1153-1164. doi: 10.1177/03635465241234258. Epub 2024 Mar 12. Am J Sports Med. 2024. PMID: 38476016 Free PMC article.
-
High Risk of Conversion to THA After Femoroacetabular Osteoplasty for Femoroacetabular Impingement in Patients Older than 40 Years.Clin Orthop Relat Res. 2021 May 1;479(5):1112-1118. doi: 10.1097/CORR.0000000000001554. Clin Orthop Relat Res. 2021. PMID: 33236866 Free PMC article.
-
Revision Surgery and Progression to Total Hip Arthroplasty After Surgical Correction of Femoroacetabular Impingement: A Systematic Review.Am J Sports Med. 2022 Mar;50(4):1146-1156. doi: 10.1177/03635465211011744. Epub 2021 Jun 3. Am J Sports Med. 2022. PMID: 34081552 Free PMC article.
-
Outcomes of arthroscopy of the hip for femoroacetabular impingement based on intraoperative assessment using the Outerbridge classification.Bone Joint J. 2023 Jul 1;105-B(7):751-759. doi: 10.1302/0301-620X.105B7.BJJ-2022-0989.R1. Bone Joint J. 2023. PMID: 37399116
Cited by
-
Predicting Outcomes in Hip Arthroscopy for Femoroacetabular Impingement Syndrome.Curr Rev Musculoskelet Med. 2024 Mar;17(3):59-67. doi: 10.1007/s12178-023-09880-w. Epub 2024 Jan 6. Curr Rev Musculoskelet Med. 2024. PMID: 38182802 Free PMC article. Review.
-
Evaluation of Outcomes Following Arthroscopic Treatment of Femoroacetabular Impingement Syndrome Across Different Surgeons, Surgical Techniques, and Postoperative Protocols: A Multi-institutional Study.Orthop J Sports Med. 2025 Jan 22;13(1):23259671241303766. doi: 10.1177/23259671241303766. eCollection 2025 Jan. Orthop J Sports Med. 2025. PMID: 39850775 Free PMC article.
-
A Novel Model of Hip Femoroacetabular Impingement in Immature Rabbits Reproduces the Distinctive Head-Neck Cam Deformity.Am J Sports Med. 2022 Jun;50(7):1919-1927. doi: 10.1177/03635465221090645. Epub 2022 Apr 13. Am J Sports Med. 2022. PMID: 35416068 Free PMC article.
-
Efficacy and safety of arthroscopy in femoroacetabular impingement syndrome: a systematic review and meta-analysis of randomized clinical trials.Sci Rep. 2025 Mar 5;15(1):7775. doi: 10.1038/s41598-025-91788-1. Sci Rep. 2025. PMID: 40044717 Free PMC article.
-
Efficacy and safety of arthroscopy in femoroacetabular impingement syndrome: a systematic review and meta-analysis of randomized clinical trials.Sci Rep. 2023 Oct 1;13(1):16493. doi: 10.1038/s41598-023-43441-y. Sci Rep. 2023. Retraction in: Sci Rep. 2024 Sep 3;14(1):20491. doi: 10.1038/s41598-024-71300-x. PMID: 37779117 Free PMC article. Retracted.
References
-
- Anciano Granadillo V, Cancienne JM, Gwathmey FW, Werner BC. Perioperative Opioid Analgesics and Hip Arthroscopy: Trends, Risk Factors for Prolonged Use, and Complications. Arthroscopy. 2018;34:2359-2367. - PubMed
-
- Bonazza NA, Homcha B, Liu G, Leslie DL, Dhawan A. Surgical Trends in Arthroscopic Hip Surgery Using a Large National Database. Arthroscopy. 2018;34:1825-1830. - PubMed
-
- Bozic KJ, Chan V, Valone FH, 3rd, Feeley BT, Vail TP. Trends in hip arthroscopy utilization in the United States. J Arthroplasty. 2013;28:140-143. - PubMed
-
- Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45:613-619. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
