

Inversion Recovery Susceptibility Weighted Imaging With Enhanced T2 Weighting at 3 T Improves Visualization of Subpial Cortical Multiple Sclerosis Lesions
- PMID: 32604385
- PMCID: PMC7541598
- DOI: 10.1097/RLI.0000000000000698
Inversion Recovery Susceptibility Weighted Imaging With Enhanced T2 Weighting at 3 T Improves Visualization of Subpial Cortical Multiple Sclerosis Lesions
Abstract
Objectives: Cortical demyelination is common in multiple sclerosis (MS) and can be extensive. Cortical lesions contribute to disability independently from white matter lesions and may form via a distinct mechanism. However, current magnetic resonance imaging methods at 3 T are insensitive to cortical, and especially subpial cortical, lesions. Subpial lesions are well seen on T2*-weighted imaging at 7 T, but T2*-weighted methods on 3 T scanners are limited by poor lesion-to-cortex and cerebrospinal fluid-to-lesion contrast. We aimed to develop and evaluate a cerebrospinal fluid-suppressed, T2*-weighted sequence optimized for subpial cortical lesion visualization.
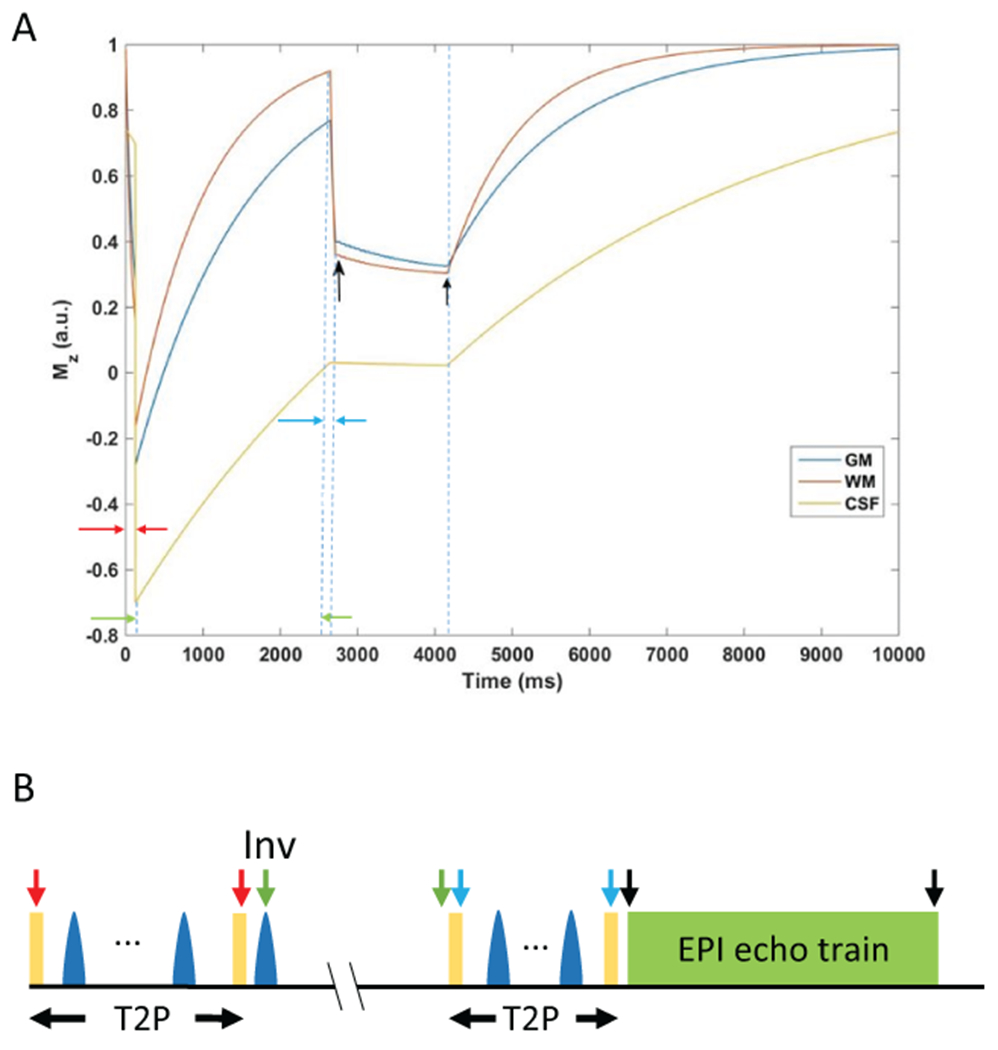
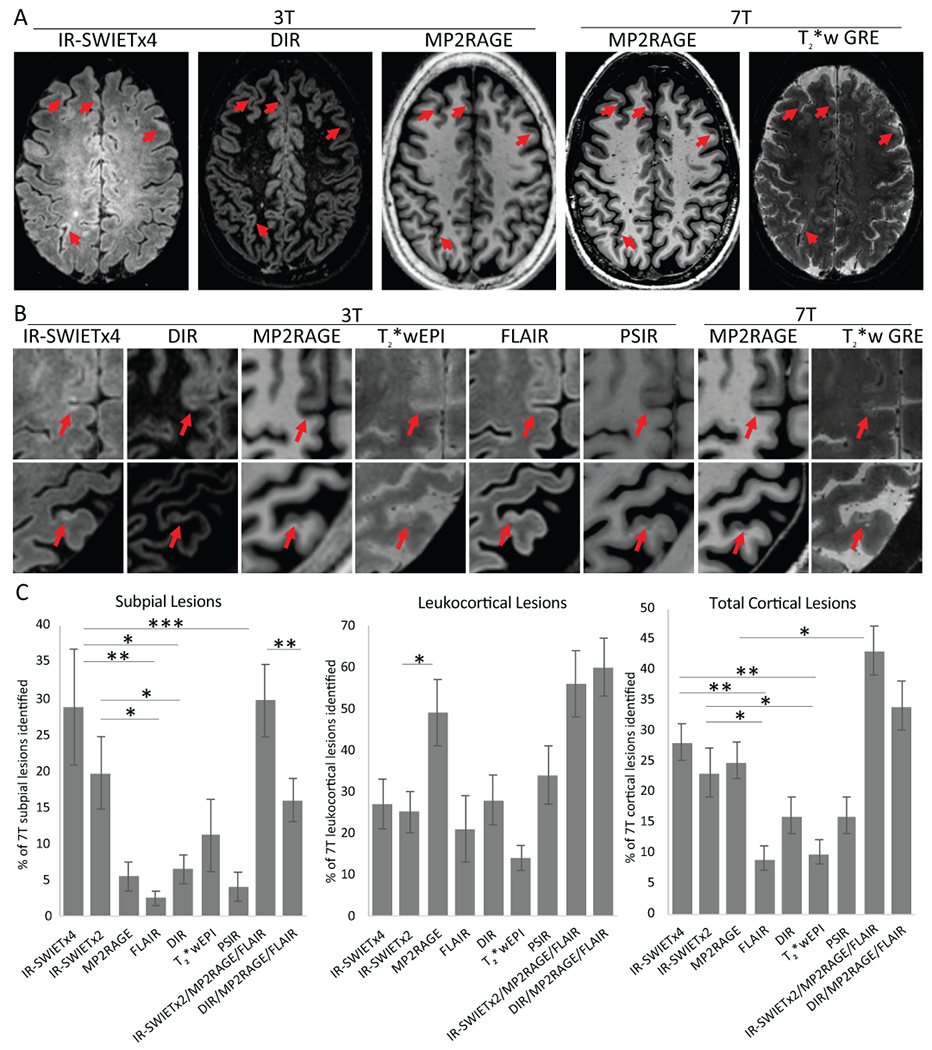
Materials and methods: We developed a new magnetic resonance imaging sequence, inversion recovery susceptibility weighted imaging with enhanced T2 weighting (IR-SWIET; 0.8 mm × 0.8 mm in plane, 0.64 mm slice thickness with whole brain coverage, acquisition time ~5 minutes). We compared cortical lesion visualization independently on IR-SWIET (median signal from 4 acquisitions), magnetization-prepared 2 rapid acquisition gradient echoes (MP2RAGE), double inversion recovery (DIR), T2*-weighted segmented echo-planar imaging, and phase-sensitive inversion recovery images for 10 adults with MS. We also identified cortical lesions with a multicontrast reading of IR-SWIET (median of 2 acquisitions), MP2RAGE, and fluid-attenuated inversion recovery (FLAIR) images for each case. Lesions identified on 3 T images were verified on "gold standard" 7 T T2* and MP2RAGE images.
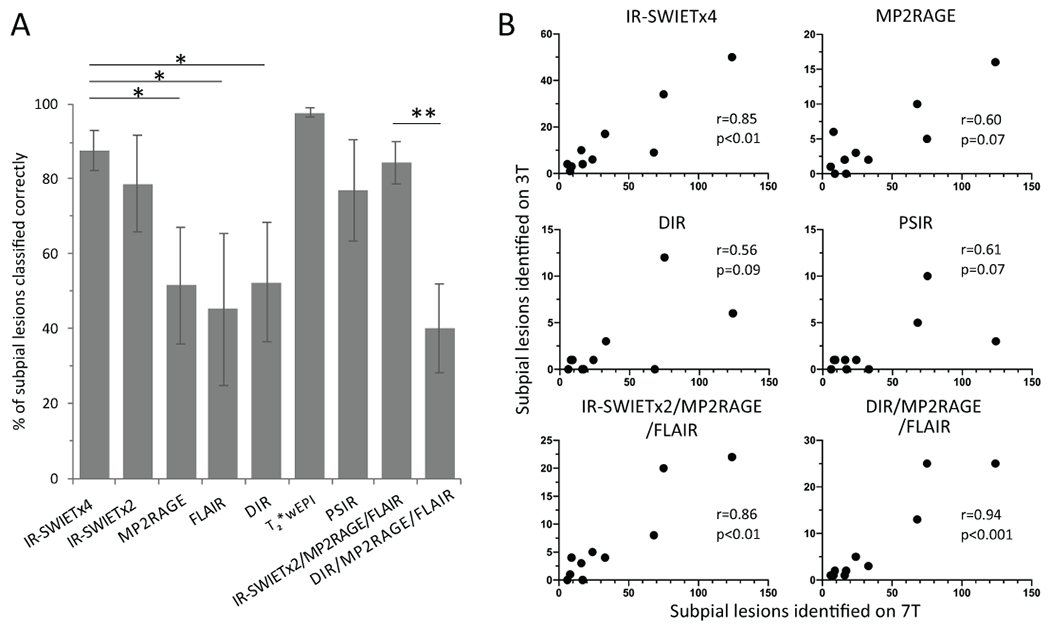
Results: Cortical, and particularly subpial, lesions appeared much more conspicuous on IR-SWIET compared with other 3 T methods. A total of 101 true-positive subpial lesions were identified on IR-SWIET (average per-participant sensitivity vs 7 T, 29% ± 8%) versus 36 on MP2RAGE (5% ± 2%; comparison to IR-SWIET sensitivity, P = 0.07), 17 on FLAIR (2% ± 1%; P < 0.05), 28 on DIR (6% ± 2%; P < 0.05), 42 on T2*-weighted segmented echo-planar imaging (11% ± 5%; P < 0.05), and 13 on phase-sensitive inversion recovery (4% ± 2%; P < 0.05). When a combination of IR-SWIET, MP2RAGE, and FLAIR images was used, a total of 147 subpial lesions (30% ± 5%) were identified versus 83 (16% ± 3%, P < 0.01) on a combination of DIR, MP2RAGE, and FLAIR. More cases had at least 1 subpial lesion on IR-SWIET, and IR-SWIET improved cortical lesion subtyping accuracy and correlation with 7 T subpial lesion number.
Conclusions: Subpial lesions are better visualized on IR-SWIET compared with other 3 T methods. A 3 T protocol combining IR-SWIET with MP2RAGE, in which leukocortical lesions are well seen, improves cortical lesion visualization over existing approaches. Therefore, IR-SWIET may enable improved MS diagnostic specificity and a better understanding of the clinical implications of cortical demyelination.
Figures
References
-
- Bo L, Vedeler CA, Nyland HI, et al. Subpial demyelination in the cerebral cortex of multiple sclerosis patients. J Neuropathol Exp Neurol. 2003;62(7):723–32. - PubMed
-
- Calabrese M, Agosta F, Rinaldi F, et al. Cortical lesions and atrophy associated with cognitive impairment in relapsing-remitting multiple sclerosis. Arch Neurol. 2009;66(9):1144–50. - PubMed
-
- Calabrese M, Poretto V, Favaretto A, et al. Cortical lesion load associates with progression of disability in multiple sclerosis. Brain. 2012;135(Pt 10):2952–61. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
