

Changes in heart morphometric parameters over the course of a monocrotaline-induced pulmonary arterial hypertension rat model
- PMID: 32605656
- PMCID: PMC7325143
- DOI: 10.1186/s12967-020-02440-7
Changes in heart morphometric parameters over the course of a monocrotaline-induced pulmonary arterial hypertension rat model
Abstract
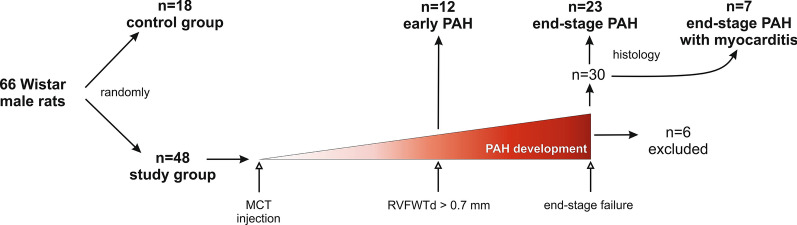
Background: Aim of this study was to assess changes in cardiac morphometric parameters at different stages of pulmonary arterial hypertension (PAH) using a monocrotaline-induced rat model.
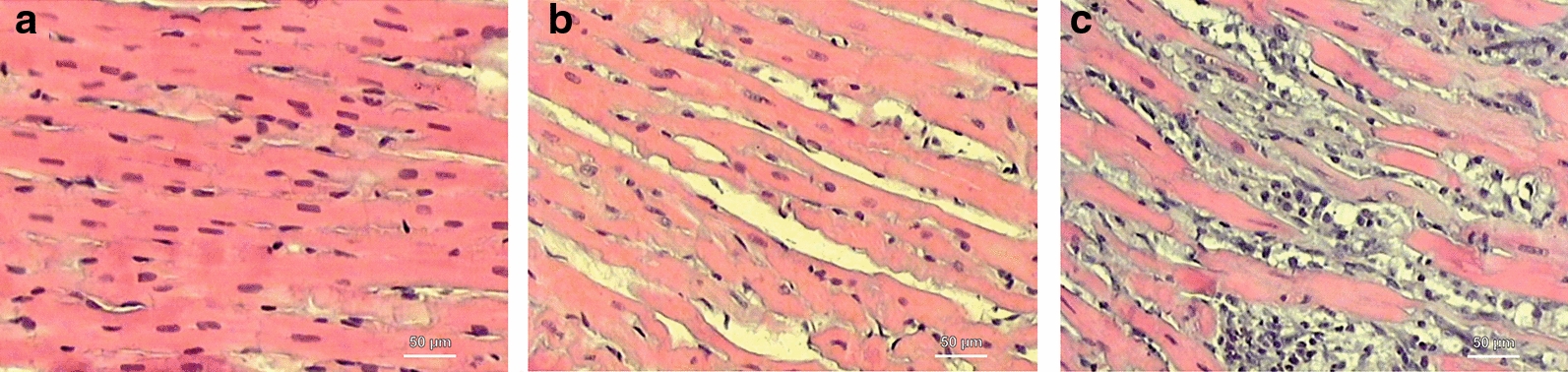
Methods: Four groups were distinguished: I-control, non-PAH (n = 18); II-early PAH (n = 12); III-end-stage PAH (n = 23); and IV-end-stage PAH with myocarditis (n = 7).
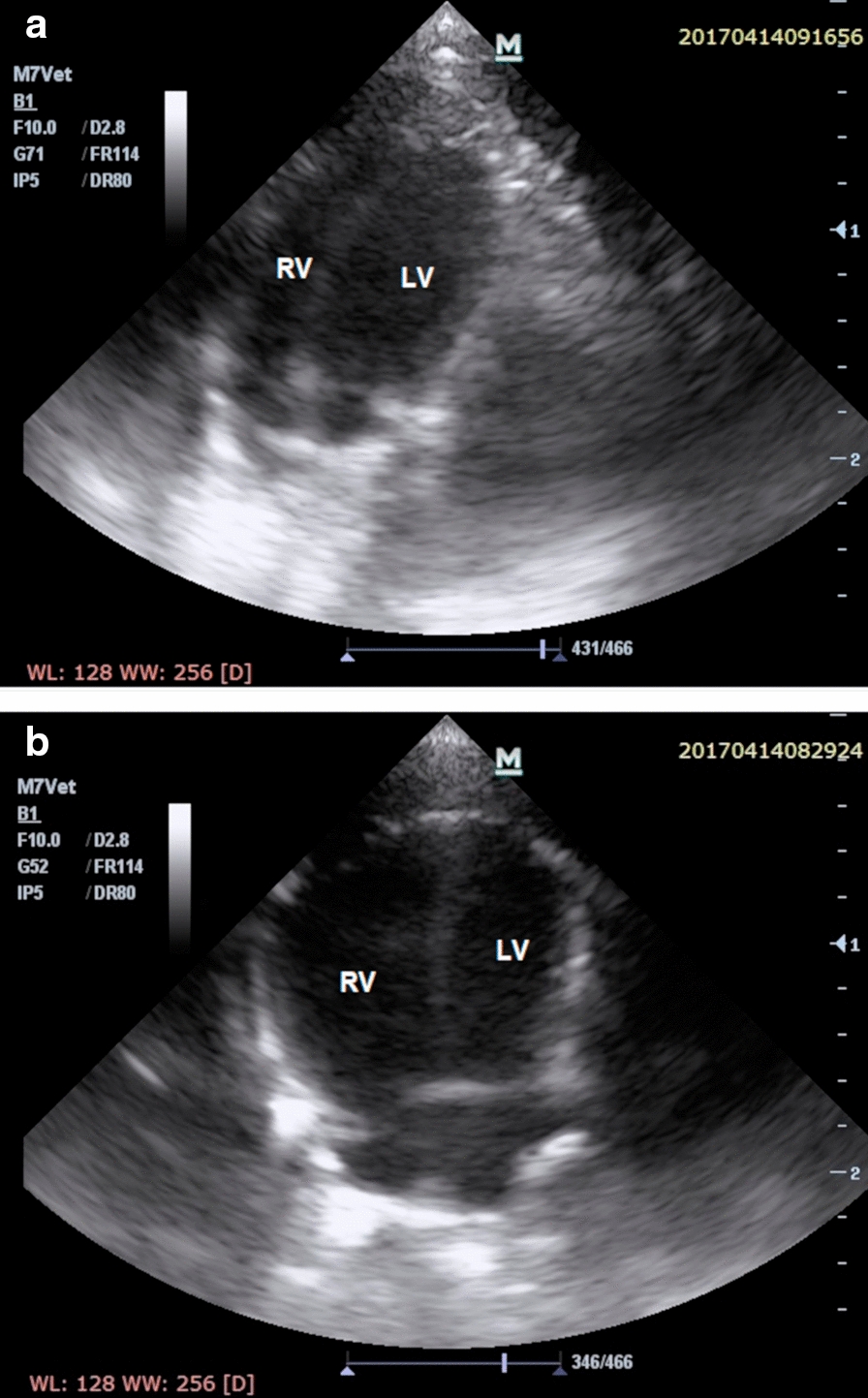
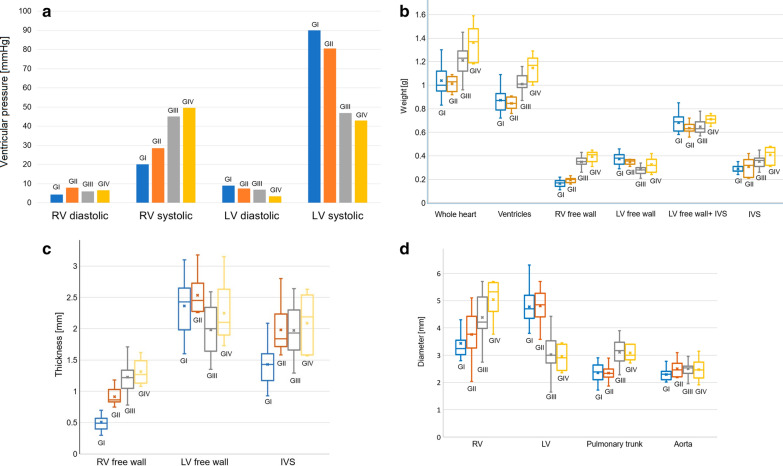
Results: Performed over the course of PAH in vivo echocardiography showed significant thickening of the right ventricle free wall (end-diastolic dimension), tricuspid annular plane systolic excursion reduction and decrease in pulmonary artery acceleration time normalized to cycle length. No differences in end-diastolic left ventricle free wall thickness measured in echocardiography was observed between groups. Significant increase of right ventricle and decrease of left ventricle systolic pressure was observed over the development of PAH. Thickening and weight increase (241.2% increase) of the right ventricle free wall and significant dilatation of the right ventricle was observed over the course of PAH (p < 0.001). Reduction in the left ventricle free wall thickness was also observed in end-stage PAH (p < 0.001). Significant trend in the left ventricle free wall weight decrease was observed over the course of PAH (p < 0.001, 24.3% reduction). Calculated right/left ventricle free wall weight ratio gradually increased over PAH stages (p < 0.001). The reduction of left ventricle diameter was observed in rats with end-stage PAH both with and without myocarditis (p < 0.001).
Conclusions: PAH leads to multidimensional changes in morphometric cardiac parameters. Right ventricle morphological and functional failure develop gradually from early stage of PAH, while left ventricle changes develop at the end stages of PAH.
Keywords: Cardiac remodelling; Left ventricle mass loss; Monocrotaline-induced PAH; Pulmonary hypertension; Right ventricular failure.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Rain S, Handoko ML, Vonk Noordegraaf A, Bogaard HJ, van der Velden J, de Man FS. Pressure-overload-induced right heart failure. Pflügers Arch Eur J Physiol. 2014;466(6):1055–1063. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
