

Severe Hemorrhage Associated With Oral Anticoagulants
- PMID: 32605708
- PMCID: PMC7358793
- DOI: 10.3238/arztebl.2020.0312
Severe Hemorrhage Associated With Oral Anticoagulants
Abstract
Background: Few data have been published to date on outcomes after the common clinical experience of severe hemorrhage in orally anticoagulated patients.
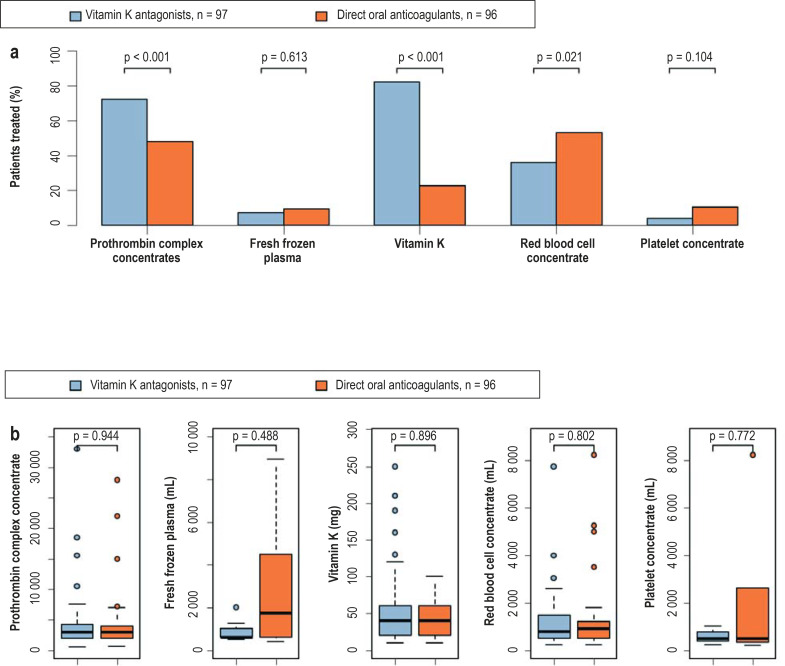
Methods: A prospective, multicenter observational study was carried out to investigate outcomes and management in a series of consecutive patients who sustained a severe hemorrhage under treatment with vitamin K antagonists (VKA) or direct oral anticoagulant drugs (DOAC). The primary endpoint was in-hospital death up to and including day 30 after hospital admission. The secondary endpoints were the duration of bleeding, in-hospital death due to hemorrhage (as defined by the study physician examining the patient's records), the use of antagonists, the extent of supportive measures used to stop the hemorrhage, and an assessment of causality. Consecutive patients were recruited until a predefined number of patients was reached in both groups.
Results: Among 193 patients with severe hemorrhage, 97 had been taking a VKA, and 96 had been taking a DOAC. 13.0 % (95% confidence interval [8.6; 18.5]; 25/193) of the overall group patients died in the first 30 days after hospital admission, including 17.5% ([10.6; 26.6]; 17/97) in the VKA group and 8.3% ([3.7; 15.8]; 8/96) in the DOAC group (p = 0.085). The median duration of bleeding was 19.8 hours in the VKA group and 27.8 hours in the DOAC group (p = 0.632). The in-hospital mortality due to hemorrhage was higher in the VKA group than in the DOAC group (15.5% [15/97] versus 4.2% [4/97]; p = 0.014). Only the use of prothrombin complex concentrates (PCCs) lowered the median duration of hemorrhage in the two patient groups. In 35% (68/193) of the patients, the hemorrhage was caused by an external influence, most commonly a fall.
Conclusion: The in-hospital mortality was higher among patients treated with VKA than among patients treated with DOAC, although the difference failed to reach statistical significance.
Figures



Comment in
-
Bleeding During Oral Anticoagulation.Dtsch Arztebl Int. 2020 May 1;117(18):311. doi: 10.3238/arztebl.2020.0311. Dtsch Arztebl Int. 2020. PMID: 32605707 Free PMC article. No abstract available.
-
Individual Risk Factors Should Be Considered.Dtsch Arztebl Int. 2020 Oct 30;117(44):752. doi: 10.3238/arztebl.2020.0752a. Dtsch Arztebl Int. 2020. PMID: 33439826 Free PMC article. No abstract available.
-
Unsuitable Comparison.Dtsch Arztebl Int. 2020 Oct 30;117(44):752-753. doi: 10.3238/arztebl.2020.0752b. Dtsch Arztebl Int. 2020. PMID: 33439827 Free PMC article. No abstract available.
References
-
- Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883–891. - PubMed
-
- Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139–1151. - PubMed
-
- Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981–992. - PubMed
-
- Einstein investigators, Bauersachs R, Berkowitz SD, et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. 2010;363:2499–2510. - PubMed
-
- Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369:2093–2104. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical