The Lyon Consensus: Does It Differ From the Previous Ones?
- PMID: 32606254
- PMCID: PMC7329153
- DOI: 10.5056/jnm20046
The Lyon Consensus: Does It Differ From the Previous Ones?
Abstract
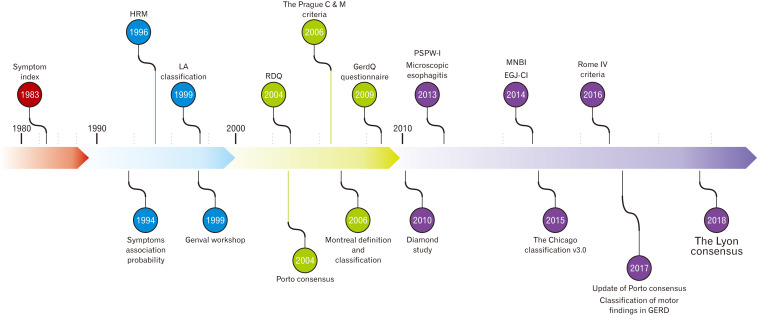
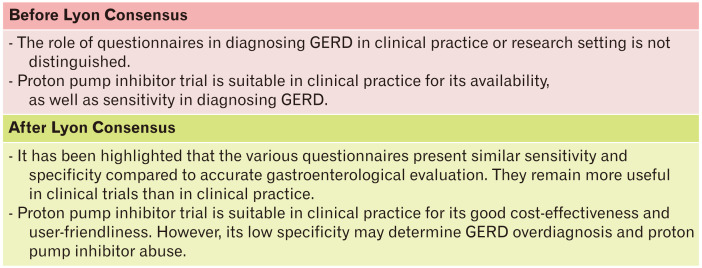
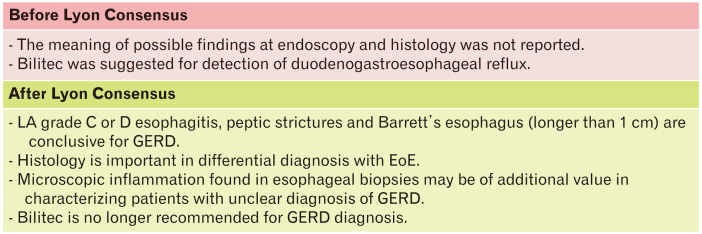
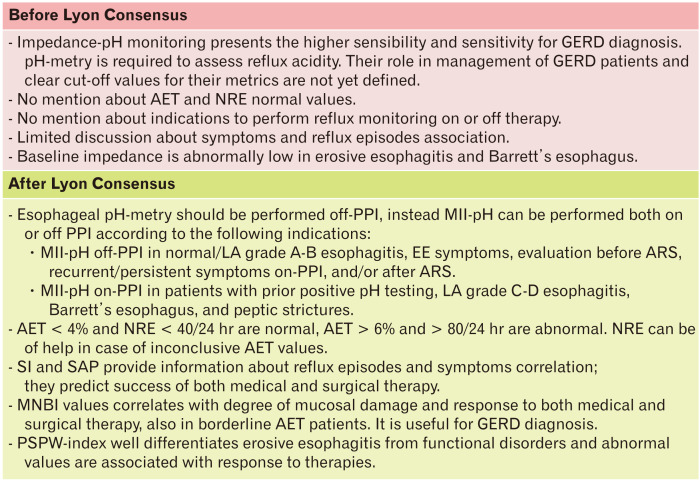
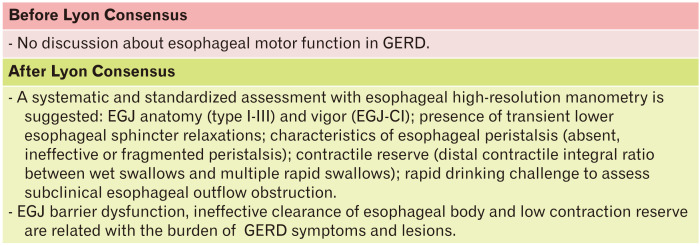
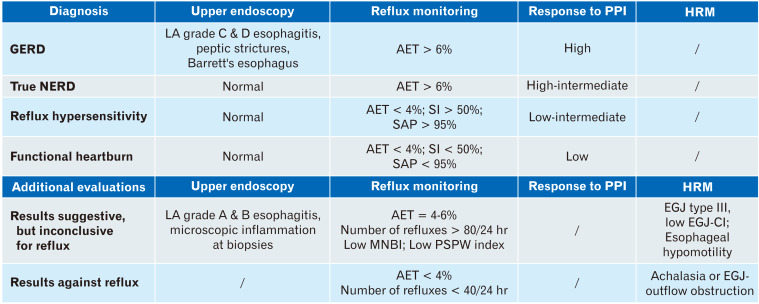
Gastroesophageal reflux disease (GERD) is a complex disorder with heterogeneous symptoms and a multifaceted pathogenetic basis, which prevent a simple diagnostic algorithm or any categorical classification. Clinical history, questionnaires and response to proton pump inhibitor (PPI) therapy are insufficient tools to make a conclusive diagnosis of GERD and further investigations are frequently required. The Lyon Consensus goes beyond the previous classifications and defines endoscopic and functional parameters able to establish the presence of GERD. Evidences for reflux include high-grade erosive esophagitis, Barrett's esophagus, and peptic strictures at endoscopy as well as esophageal acid exposure time > 6% on pH-metry or combined pH-impedance monitoring. Even if a normal endoscopy does not exclude GERD, its combination with distal acid exposure time < 4% on off-PPI pH-impedance monitoring provides sufficient evidence refuting this diagnosis. Reflux-symptom association on pH-monitoring provides supportive evidence for reflux-triggered symptoms and may predict a better treatment outcome, when present. Also recommendations to perform pH-impedance "on" or "off" PPI are well depicted. When endoscopy and pH-metry or combined pH-impedance monitoring are inconclusive, adjunctive evidence from biopsy findings (eg, microscopic esophagitis), high-resolution manometry (ie, ineffective esophagogastric barrier and esophageal body hypomotility), and novel impedance metrics, such as mean nocturnal baseline impedance and post-reflux swallow-induced peristaltic wave index, can contribute to better identify patients with GERD. Definition of individual patient phenotype, based on the level of refluxate exposure, mechanism of reflux, efficacy of clearance, underlying anatomy of the esophagogastric junction, and clinical presentation, will lead to manage GERD patients with a tailored approach chosen among different types of therapy.
Keywords: Endoscopy; Esophagitis; Gastroesophageal reflux; Manometry; Proton pump inhibitors.
Conflict of interest statement
Figures
References
Publication types
LinkOut - more resources
Full Text Sources