

Detection of Cell-Dissociated Non-Typeable Haemophilus influenzae in the Airways of Patients with Chronic Obstructive Pulmonary Disease
- PMID: 32606645
- PMCID: PMC7297347
- DOI: 10.2147/COPD.S247130
Detection of Cell-Dissociated Non-Typeable Haemophilus influenzae in the Airways of Patients with Chronic Obstructive Pulmonary Disease
Abstract
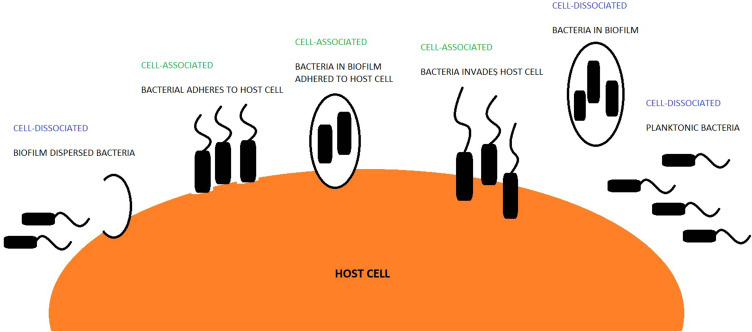
Background: Non-typeable Haemophilus influenzae (NTHi) is the most commonly found pathogen in the lower respiratory airways of patients with COPD. NTHi is predominantly regarded as an intracellular pathogen; however, like most pathogens, it can exist and co-exist in two broad forms: cell-associated (intracellularly or adhered to cells) or cell-dissociated (biofilm dispersed or planktonic). We sought to investigate if cell-dissociated NTHi can be detected from the sputum of COPD patients and assess this relationship to disease severity and airway inflammation.
Methods: DNA was extracted from the sputum plug and cell-free supernatant to quantify absolute (cell-associated and cell-dissociated NTHi) and cell-dissociated NTHi, respectively, from 87 COPD subjects attending an observational longitudinal COPD exacerbation study. NTHi was quantified using TaqMan hydrolysis probes, targeting the OMP P6 gene using qPCR.
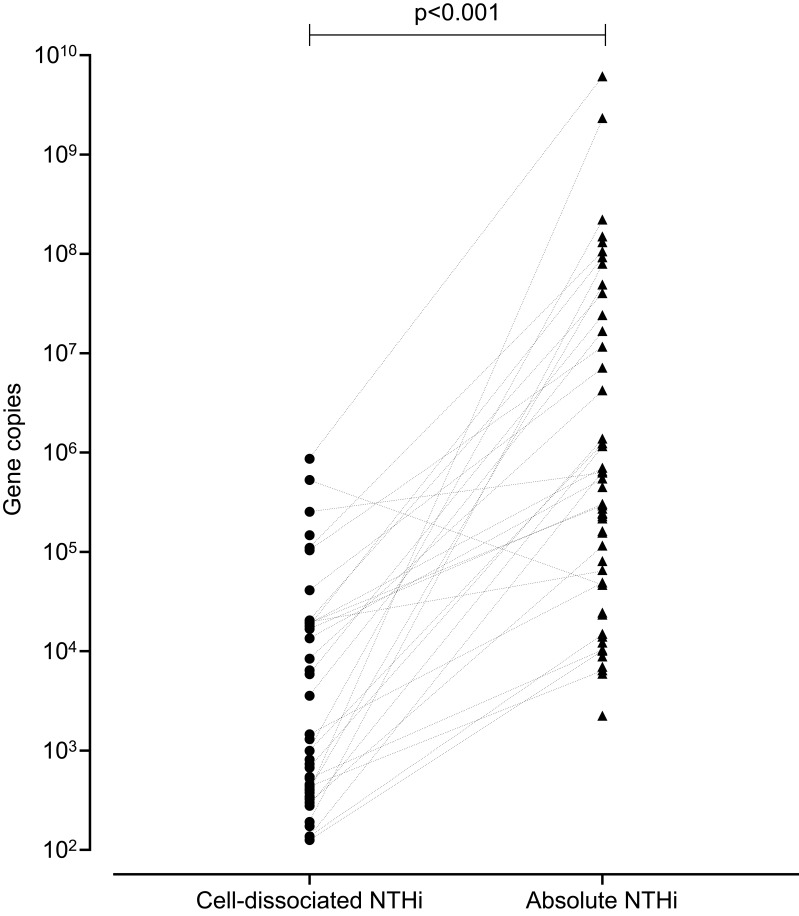
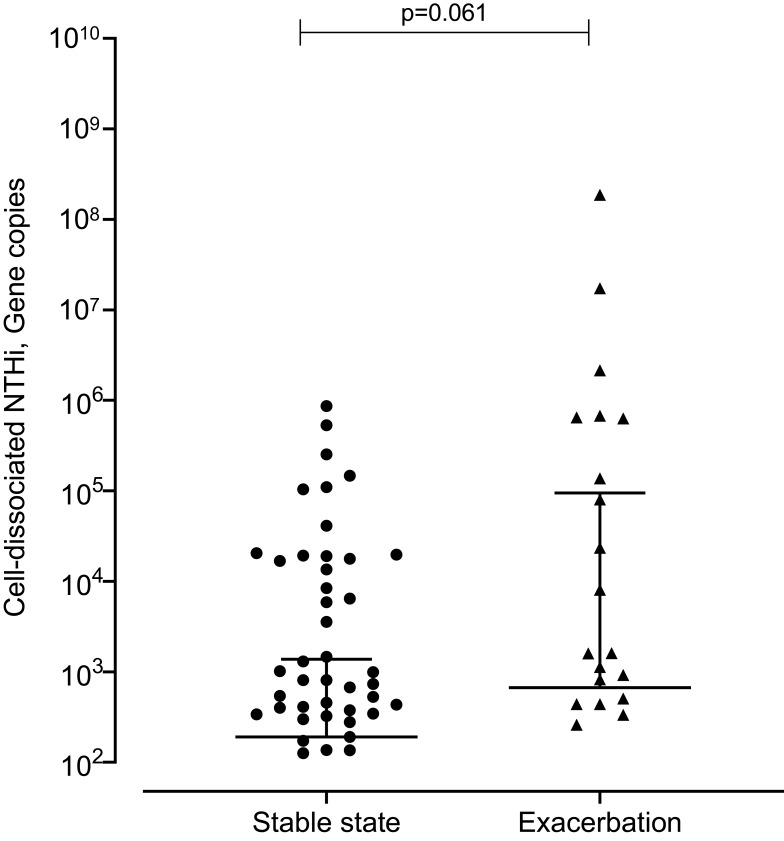
Results: At stable state cell-dissociated NTHi was detected 56% of subjects with a median (IQR) of 9.95x102 gene copies (1.26x102 to 1.90x104). Cell-dissociated NTHi correlated with absolute NTHi levels (r=0.34, p<0.01) but not airway inflammation or spirometry at stable state. At exacerbation, cell-dissociated NTHi correlated with lung function (FEV1 r=0.629, p=0.005; FEV1%predicted r=0.564, p=0.015; FVC r=0.476 p=0.046) and sputum neutrophilic inflammation (% neutrophils r=0.688, p=0.002; total neutrophils r=0.518, p=0.028).
Conclusion: In patients with COPD, NTHi can exist in both cell-associated and cell-dissociated forms. Cell-dissociated NTHi is associated with neutrophilic airway inflammation during exacerbations of COPD and may be a driving factor in worsening lung function during these episodes.
Keywords: COPD; NTHi; infection; neutrophils.
© 2020 Thulborn et al.
Conflict of interest statement
CEB was funded by a Wellcome Trust Senior Fellowship. MB was funded by a National Institute for Health Research (NIHR) Fellowship. MB has received travel support from AstraZeneca, Boehringer Ingelheim and GlaxoSmithKline and consultancy honoraria outside the submitted work from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline and Pfizer. CEB has received grant support and consultancy honoraria outside the submitted work from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Medimmune, Novartis and Roche. IDP has received grant support and consultancy honoraria outside the submitted work from Aerocrine, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline and Novartis. The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Lung mucosal immunity to NTHi vaccine antigens: Antibodies in sputum of chronic obstructive pulmonary disease patients.Hum Vaccin Immunother. 2024 Dec 31;20(1):2343544. doi: 10.1080/21645515.2024.2343544. Epub 2024 Apr 24. Hum Vaccin Immunother. 2024. PMID: 38655676 Free PMC article. Clinical Trial.
-
Relationships between Mucosal Antibodies, Non-Typeable Haemophilus influenzae (NTHi) Infection and Airway Inflammation in COPD.PLoS One. 2016 Nov 29;11(11):e0167250. doi: 10.1371/journal.pone.0167250. eCollection 2016. PLoS One. 2016. PMID: 27898728 Free PMC article.
-
The Interplay Between Immune Response and Bacterial Infection in COPD: Focus Upon Non-typeable Haemophilus influenzae.Front Immunol. 2018 Nov 5;9:2530. doi: 10.3389/fimmu.2018.02530. eCollection 2018. Front Immunol. 2018. PMID: 30455693 Free PMC article. Review.
-
Ex-vivo RNA expression analysis of vaccine candidate genes in COPD sputum samples.Respir Res. 2023 Oct 5;24(1):243. doi: 10.1186/s12931-023-02525-z. Respir Res. 2023. PMID: 37798723 Free PMC article.
-
The Role of Non-Typeable Haemophilus influenzae Biofilms in Chronic Obstructive Pulmonary Disease.Front Cell Infect Microbiol. 2021 Aug 4;11:720742. doi: 10.3389/fcimb.2021.720742. eCollection 2021. Front Cell Infect Microbiol. 2021. PMID: 34422683 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
