

Cerebral Palsy: Current Opinions on Definition, Epidemiology, Risk Factors, Classification and Treatment Options
- PMID: 32606703
- PMCID: PMC7297454
- DOI: 10.2147/NDT.S235165
Cerebral Palsy: Current Opinions on Definition, Epidemiology, Risk Factors, Classification and Treatment Options
Abstract
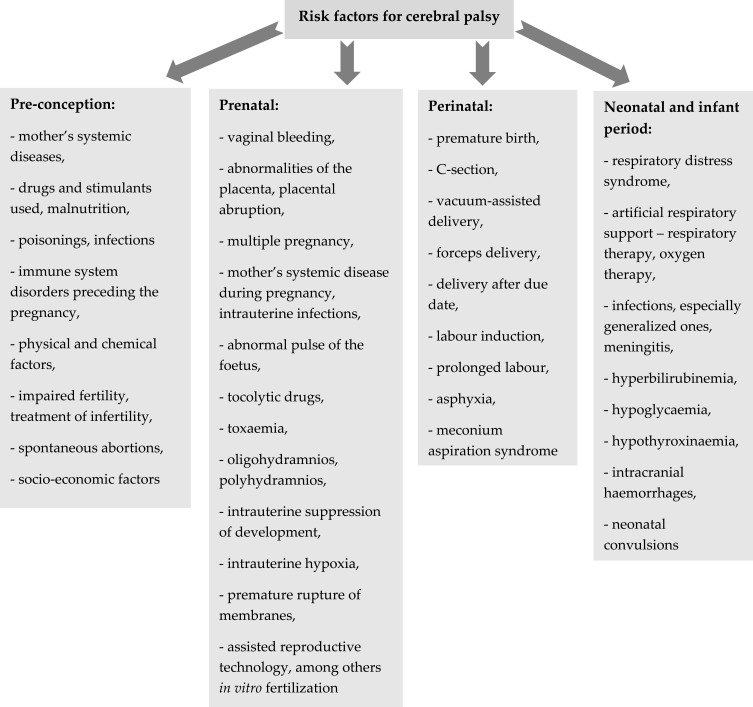
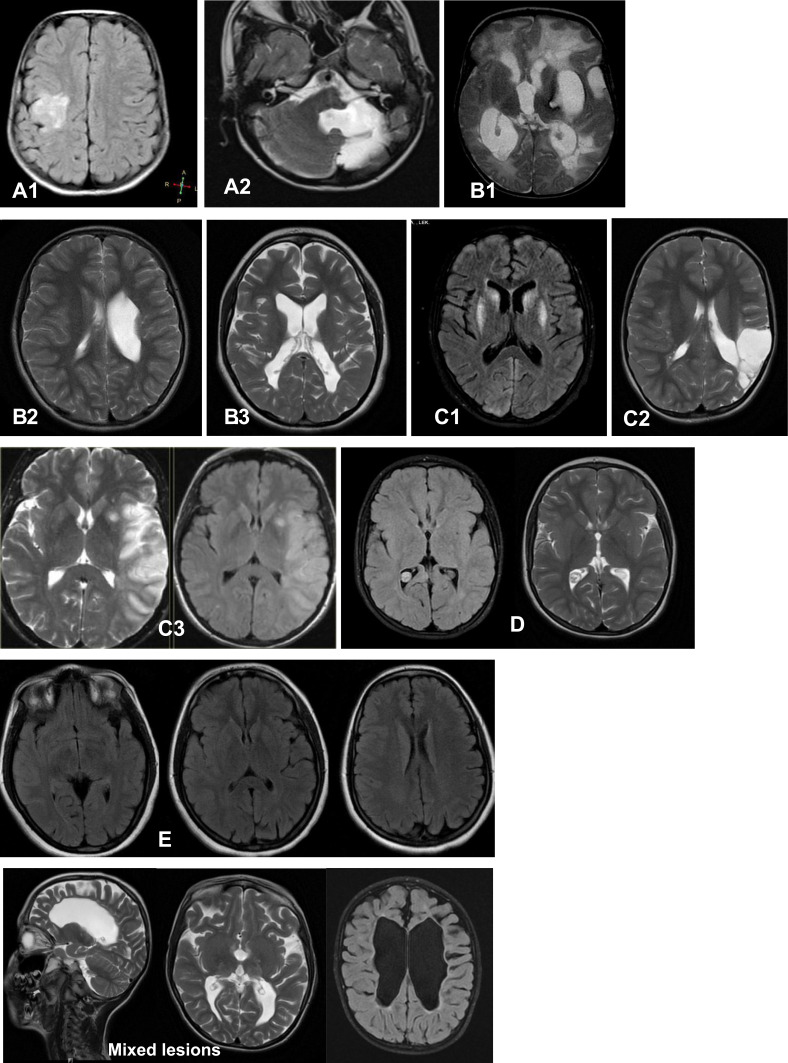
Cerebral palsy (CP) is one of the most frequent causes of motor disability in children. According to the up-to-date definition, CP is a group of permanent disorders of the development of movement and posture, causing activity limitations that are attributed to non-progressive disturbances that occurred in the developing foetal or infant brain. The CP definition has evolved over time; the problem is aetiologically and clinically very heterogeneous. According to European data, the average frequency of CP is 2.08 per 1000 live births, but in the group of children born with a body weight below 1500 g, the frequency is 70 times higher when compared with the group of children with a body weight over 2500 g at birth. The risk factors for CP can be divided into pre-conception, prenatal, perinatal and postnatal ones. CP commonly co-exists with epilepsy, in particular drug-resistant epilepsy, but also with mental retardation, visual and hearing impairment, as well as feeding and behavioral disorders. The degree of motor problem varies from mild to very severe making the child totally dependent on caregivers. Cerebral palsy is divided into forms depending on the type of motor disorders which dominate the clinical presentation; the traditional classifications by Ingram and Hagberg have now been replaced by the Surveillance of Cerebral Palsy in Europe classification which divides CP into spastic, dyskinetic and ataxic forms. Although cerebral palsy is a clinical diagnosis, modern diagnostic imaging provides information that allows the division of the results of magnetic resonance imaging in children with cerebral palsy into five groups according to the magnetic resonance imaging classification system. Just as the clinical presentation and the factors predisposing for CP are very diverse, treatment is also a very complex problem. Modern treatment of spasticity includes both botulinum toxin therapies and surgical techniques, eg, rhizotomy. The authors present current views on definitions, risk factors, diagnostics and treatment of CP as well as comorbid problems, eg, drug-resistant epilepsy.
Keywords: CP; cerebral palsy; comorbidities; epilepsy; malnutrition; mental retardation; risk factors; treatment.
© 2020 Sadowska et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
References
-
- Mac Keith RC, Mackenzie I, Polani P. The Little Club. Memorandum on terminology and classification of “cerebral palsy”. Dev Med Child Neurol. 1959;1:27–35. doi: 10.1111/j.1469-8749.1959.tb08073.x - DOI
Publication types
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
