

Comprehensive treatment of rare multiple endocrine neoplasia type 1: A case report
- PMID: 32607345
- PMCID: PMC7322426
- DOI: 10.12998/wjcc.v8.i12.2647
Comprehensive treatment of rare multiple endocrine neoplasia type 1: A case report
Abstract
Background: Multiple endocrine neoplasia type 1 (MEN1) is a rare hereditary disorder caused by mutations of the MEN1 gene. It is characterized by hyperparathyroidism and involves the pancreas, anterior pituitary, duodenum, and adrenal gland. Here, we report a 40-year-old male patient with MEN1 who first manifested as thymic carcinoid, then primary hyperparathyroidism and prolactinoma, and a decade later pancreatic neuroendocrine tumor.
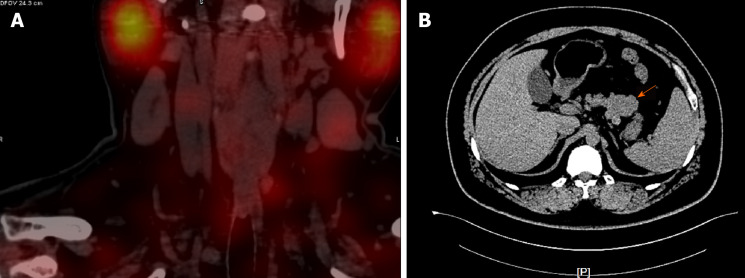
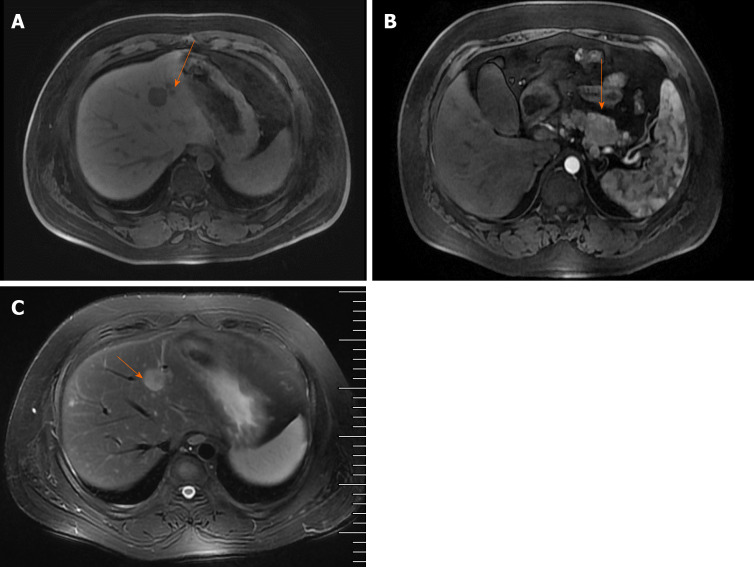
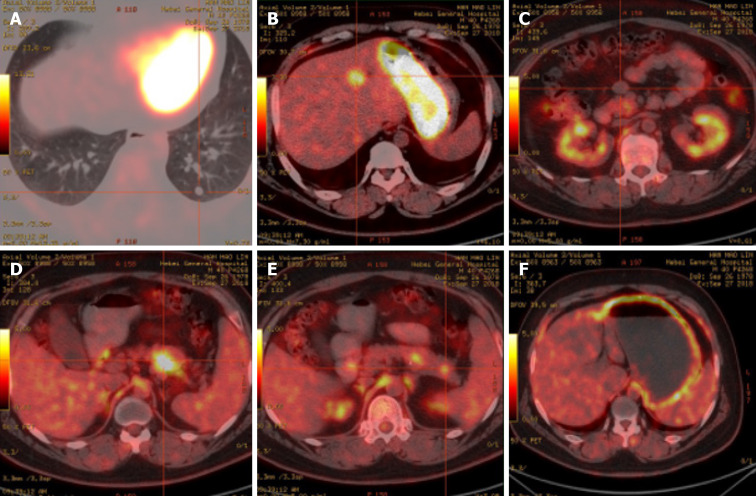
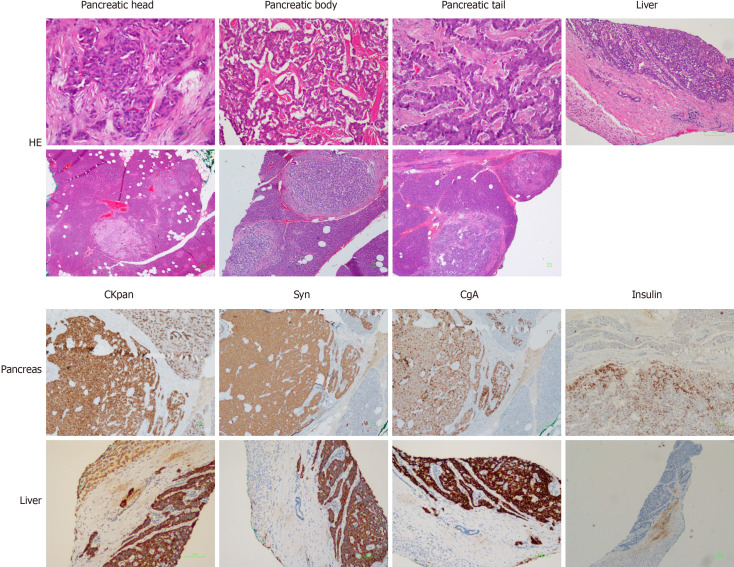
Case summary: The patient underwent a thymectomy because of the thymic carcinoid 10 years prior and a prolactinoma resection 2 years prior. His sister suffered from prolactinoma. His parents displayed a typical triad of amenorrhea, galactorrhea, and infertility. Computed tomography revealed a strong signal in the upper portion of the left lobes and posterior portion of the right lobes of the thyroid and irregular soft tissue densities of the pancreatic body. Positron emission tomography/computed tomography imaging further showed strong 18F-flurodeoxyglucose uptake in the tail of the pancreatic body and segment IV of the liver. The patient underwent pancreatic body tail resection, pancreatic head mass enucleation, and ultrasound-guided radio-frequency ablation for liver cancer. Pathology results reported neuroendocrine tumor grade 2. Whole exome sequencing revealed a verified pathogenic mutation c.378G>A (p.Trp126*) in the MEN1 gene. The diagnosis of MEN1 was confirmed. At the 1.5-year follow-up, the patient appeared healthy without any sign of reoccurrence.
Conclusion: The present case may add some insight into the diagnosis and treatment of patients with MEN1.
Keywords: Case report; Multiple endocrine neoplasia type 1; Neuroendocrine tumor; Pancreas; Thymic carcinoid; Tumor.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: We declare that we have no conflict of interest.
Figures
Similar articles
-
Thymic Carcinoid as the First Manifestation of Multiple Endocrine Neoplasia Type 1 Syndrome: A Case Report and Review of the Literature.Ann Clin Lab Sci. 2020 Nov;50(6):825-833. Ann Clin Lab Sci. 2020. PMID: 33334800 Review.
-
Thymic carcinoid in a patient with multiple endocrine neoplasia type 1: report of a case.Surg Today. 2001;31(5):428-32. doi: 10.1007/s005950170134. Surg Today. 2001. PMID: 11381507
-
Atypical ovarian carcinoid tumor with widespread skeletal metastases: a case report of multiple endocrine neoplasia type 1 in a young woman.BMC Cancer. 2019 Nov 14;19(1):1107. doi: 10.1186/s12885-019-6332-7. BMC Cancer. 2019. PMID: 31727021 Free PMC article.
-
Multiple Endocrine Neoplasia Type 1: A Case Report With Review of Imaging Findings.Ochsner J. 2018 Summer;18(2):170-175. doi: 10.31486/toj.17.0019. Ochsner J. 2018. PMID: 30258300 Free PMC article.
-
Diagnosis and treatment of multiple endocrine neoplasia type 1 (MEN1).Minerva Endocrinol. 2013 Mar;38(1):17-28. Minerva Endocrinol. 2013. PMID: 23435440 Review.
Cited by
-
Importance of early detection in multiple endocrine neoplasia type 1: Clinical insights and future directions.World J Gastrointest Oncol. 2025 Apr 15;17(4):100013. doi: 10.4251/wjgo.v17.i4.100013. World J Gastrointest Oncol. 2025. PMID: 40235881 Free PMC article.
-
Turning Points in Cross-Disciplinary Perspective of Primary Hyperparathyroidism and Pancreas Involvements: Hypercalcemia-Induced Pancreatitis, MEN1 Gene-Related Tumors, and Insulin Resistance.Int J Mol Sci. 2024 Jun 8;25(12):6349. doi: 10.3390/ijms25126349. Int J Mol Sci. 2024. PMID: 38928056 Free PMC article. Review.
References
-
- Thakker RV, Newey PJ, Walls GV, Bilezikian J, Dralle H, Ebeling PR, Melmed S, Sakurai A, Tonelli F, Brandi ML Endocrine Society. Clinical practice guidelines for multiple endocrine neoplasia type 1 (MEN1) J Clin Endocrinol Metab. 2012;97:2990–3011. - PubMed
-
- Kim JY, Hong SM, Ro JY. Recent updates on grading and classification of neuroendocrine tumors. Ann Diagn Pathol. 2017;29:11–16. - PubMed
-
- Thakker RV. Multiple endocrine neoplasia type 1 (MEN1) Best Pract Res Clin Endocrinol Metab. 2010;24:355–370. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
