

This is a preprint.
COVID-19 Outpatient Screening: a Prediction Score for Adverse Events
- PMID: 32607523
- PMCID: PMC7325189
- DOI: 10.1101/2020.06.17.20134262
COVID-19 Outpatient Screening: a Prediction Score for Adverse Events
Update in
-
CoVA: An Acuity Score for Outpatient Screening that Predicts Coronavirus Disease 2019 Prognosis.J Infect Dis. 2021 Jan 4;223(1):38-46. doi: 10.1093/infdis/jiaa663. J Infect Dis. 2021. PMID: 33098643 Free PMC article.
Abstract
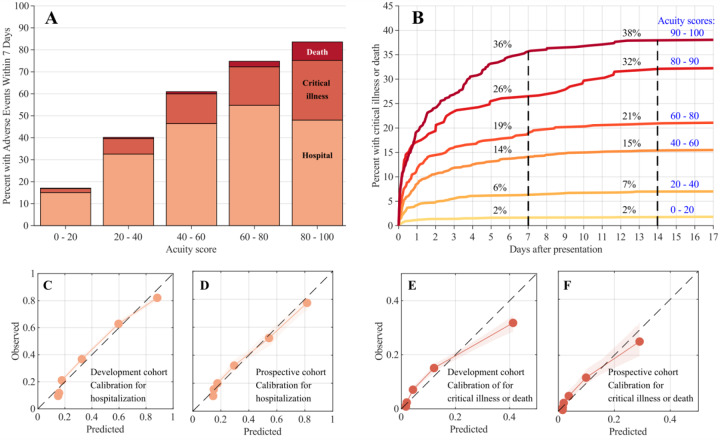
Background: We sought to develop an automatable score to predict hospitalization, critical illness, or death in patients at risk for COVID-19 presenting for urgent care during the Massachusetts outbreak.
Methods: Single-center study of adult outpatients seen in respiratory illness clinics (RICs) or the emergency department (ED), including development (n = 9381, March 7-May 2) and prospective (n = 2205, May 3-14) cohorts. Data was queried from Partners Enterprise Data Warehouse. Outcomes were hospitalization, critical illness or death within 7 days. We developed the COVID-19 Acuity Score (CoVA) using automatically extracted data from the electronic medical record and learning-to-rank ordinal logistic regression modeling. Calibration was assessed using predicted-to-observed event ratio (E/O). Discrimination was assessed by C-statistics (AUC).
Results: In the development cohort, 27.3%, 7.2%, and 1.1% of patients experienced hospitalization, critical illness, or death, respectively; and in the prospective cohort, 26.1%, 6.3%, and 0.5%. CoVA showed excellent performance in the development cohort (concurrent validation) for hospitalization (E/O: 1.00, AUC: 0.80); for critical illness (E/O: 1.00, AUC: 0.82); and for death (E/O: 1.00, AUC: 0.87). Performance in the prospective cohort (prospective validation) was similar for hospitalization (E/O: 1.01, AUC: 0.76); for critical illness (E/O 1.03, AUC: 0.79); and for death (E/O: 1.63, AUC=0.93). Among 30 predictors, the top five were age, diastolic blood pressure, blood oxygen saturation, COVID-19 testing status, and respiratory rate.
Conclusions: CoVA is a prospectively validated automatable score to assessing risk for adverse outcomes related to COVID-19 infection in the outpatient setting.
Conflict of interest statement
Figures
References
-
- S R, Js H, M N, et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA, 2020. Available at: https://pubmed.ncbi.nlm.nih.gov/32320003/?from_term=covid+new+york&from_.... Accessed 5 June 2020. - PMC - PubMed
-
- First Case of Covid-19 in the United States | NEJM. Available at: https://www-nejm-org.ezp-prod1.hul.harvard.edu/doi/full/10.1056/NEJMc200.... Accessed 5 June 2020. - DOI
-
- Covid-19 — Navigating the Uncharted | NEJM. N Engl J Med Available at: http://www.nejm.org/doi/10.1056/NEJMe2002387. Accessed 5 June 2020. - DOI - PMC - PubMed
-
- Wu Z, McGoogan JM. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020; - PubMed
Publication types
Grants and funding
- R01 NS105820/NS/NINDS NIH HHS/United States
- R01 AG008122/AG/NIA NIH HHS/United States
- R56 AG064027/AG/NIA NIH HHS/United States
- S10 RR023043/RR/NCRR NIH HHS/United States
- R01 NS107291/NS/NINDS NIH HHS/United States
- U01 MH093765/MH/NIMH NIH HHS/United States
- R01 NS070963/NS/NINDS NIH HHS/United States
- U01 NS086625/NS/NINDS NIH HHS/United States
- R21 EB018907/EB/NIBIB NIH HHS/United States
- R01 NS102190/NS/NINDS NIH HHS/United States
- R01 AG064027/AG/NIA NIH HHS/United States
- R01 AG016495/AG/NIA NIH HHS/United States
- T32 NS100663/NS/NINDS NIH HHS/United States
- R21 DK108277/DK/NIDDK NIH HHS/United States
- S10 RR019307/RR/NCRR NIH HHS/United States
- K23 MH115812/MH/NIMH NIH HHS/United States
- R01 EB023281/EB/NIBIB NIH HHS/United States
- RF1 AG064312/AG/NIA NIH HHS/United States
- R01 NS102574/NS/NINDS NIH HHS/United States
- R01 EB019956/EB/NIBIB NIH HHS/United States
- U01 MH117023/MH/NIMH NIH HHS/United States
- R21 NS072652/NS/NINDS NIH HHS/United States
- P30 AI060354/AI/NIAID NIH HHS/United States
- R01 EB006758/EB/NIBIB NIH HHS/United States
- P41 EB015896/EB/NIBIB NIH HHS/United States
- R01 NS083534/NS/NINDS NIH HHS/United States
- S10 RR023401/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Miscellaneous