

Relationship Between Intensive Care Unit Delirium Severity and 2-Year Mortality and Health Care Utilization
- PMID: 32607574
- PMCID: PMC7891863
- DOI: 10.4037/ajcc2020498
Relationship Between Intensive Care Unit Delirium Severity and 2-Year Mortality and Health Care Utilization
Abstract
Background: Critical care patients with delirium are at an increased risk of functional decline and mortality long term.
Objective: To determine the relationship between delirium severity in the intensive care unit and mortality and acute health care utilization within 2 years after hospital discharge.
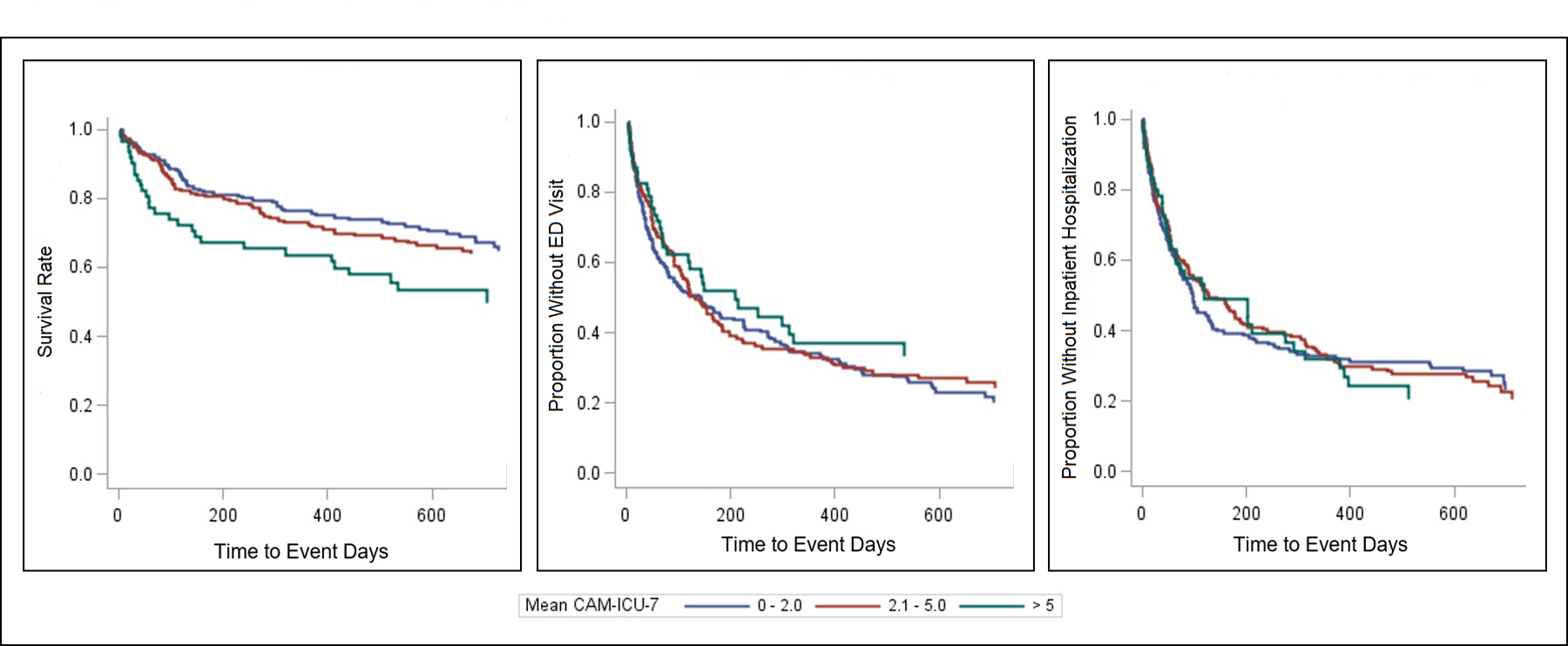
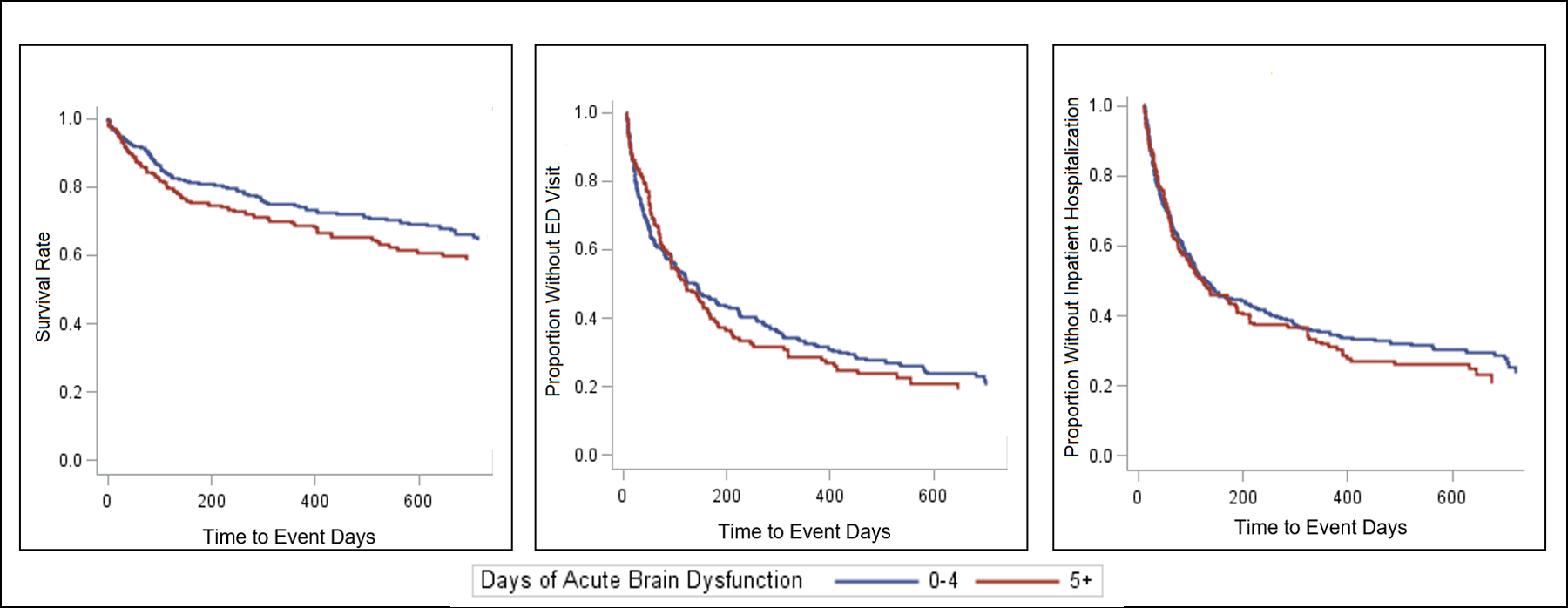
Methods: A secondary data analysis of the Pharmacological Management of Delirium and Deprescribe randomized controlled trials. Patients were assessed twice daily for delirium or coma using the Richmond Agitation-Sedation Scale and the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU). Delirium severity was measured using the CAM-ICU-7. Mean delirium severity (from time of randomization to discharge) was categorized as rapidly resolving, mild to moderate, or severe. Cox proportional hazards regression was used to model time to death, first emergency department visit, and rehospitalization. Analyses were adjusted for age, sex, race, Charlson Comorbidity Index, Acute Physiology and Chronic Health Evaluation II score, discharge location, diagnosis, and intensive care unit type.
Results: Of 434 patients, those with severe delirium had higher mortality risk than those with rapidly resolving delirium (hazard ratio 2.21; 95% CI, 1.35-3.61). Those with 5 or more days of delirium or coma had higher mortality risk than those with less than 5 days (hazard ratio 1.52; 95% CI, 1.07-2.17). Delirium severity and number of days of delirium or coma were not associated with time to emergency department visits and rehospitalizations.
Conclusion: Increased delirium severity and days of delirium or coma are associated with higher mortality risk 2 years after discharge.
© 2020 American Association of Critical-Care Nurses.
Figures
References
-
- Hshieh TT, Inouye SK, Oh ES. Delirium in the elderly. Psychiatr Clin N Am. 2018;41(1):1–17. - PubMed
-
- Ely EW, Margolin R, Francis J, et al. Evaluation of delirium in critically ill patients: validation of the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU). Crit Care Med. 2001;29(7):1370–1379. - PubMed
-
- McNicoll L, Pisani MA, Zhang Y, Ely EW, Siegel MD, Inouye SK. Delirium in the intensive care unit: occurrence and clinical course in older patients. J Am Geriatr Soc. 2003;51(5):591–598 - PubMed
Publication types
MeSH terms
Grants and funding
- P30 AG010133/AG/NIA NIH HHS/United States
- R01 AG056325/AG/NIA NIH HHS/United States
- K23 AG062555/AG/NIA NIH HHS/United States
- R01 AG056926/AG/NIA NIH HHS/United States
- R01 AG054574/AG/NIA NIH HHS/United States
- R01 HL131730/HL/NHLBI NIH HHS/United States
- R01 AG061452/AG/NIA NIH HHS/United States
- P30 HS024384/HS/AHRQ HHS/United States
- R21 AG062966/AG/NIA NIH HHS/United States
- R01 AG052493/AG/NIA NIH HHS/United States
- UL1 TR002529/TR/NCATS NIH HHS/United States
- T32 HL091816/HL/NHLBI NIH HHS/United States
- R01 AG055391/AG/NIA NIH HHS/United States
