

The concept of direct approach to lateral tibial plateau fractures and stepwise extension as needed
- PMID: 32607776
- PMCID: PMC7691307
- DOI: 10.1007/s00068-020-01422-0
The concept of direct approach to lateral tibial plateau fractures and stepwise extension as needed
Abstract
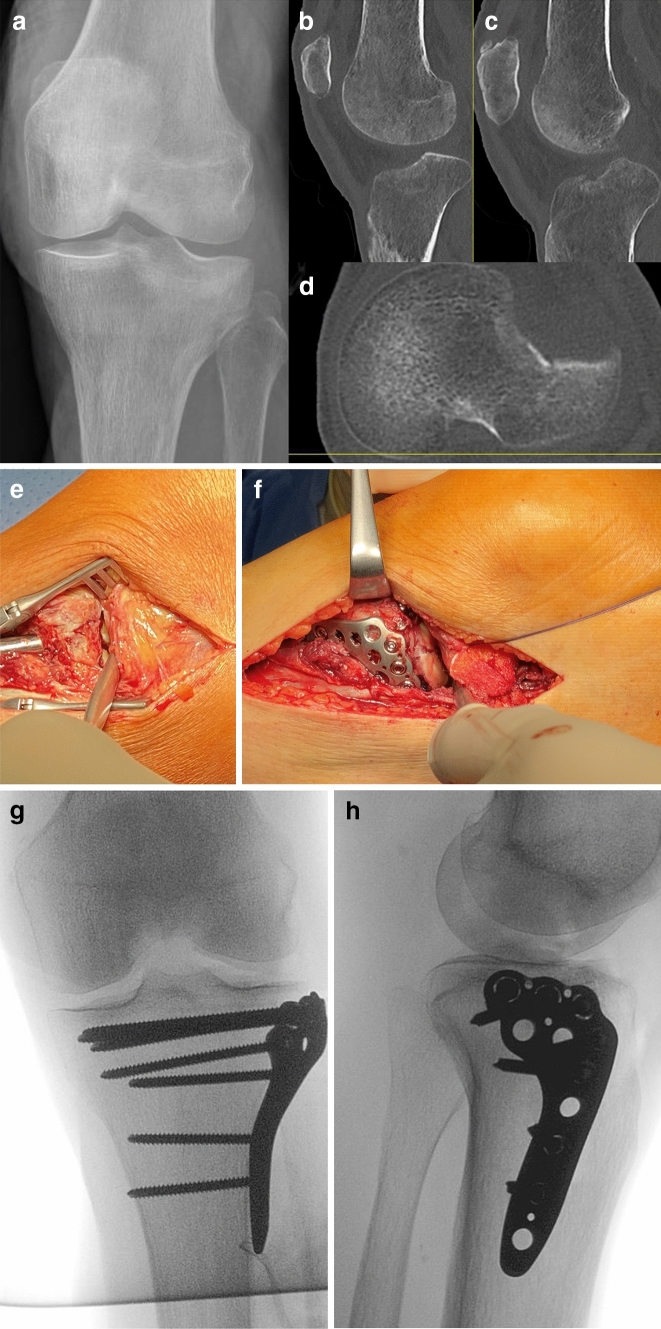
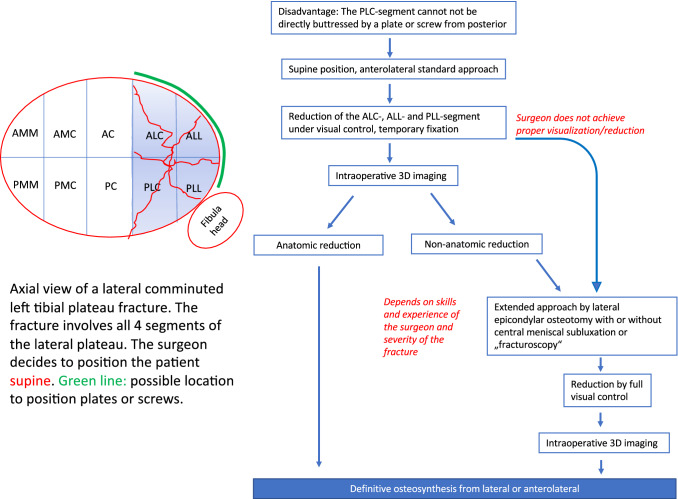
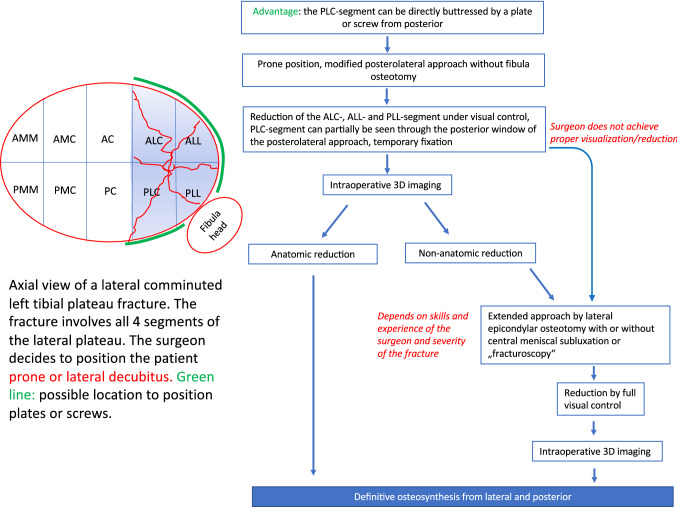
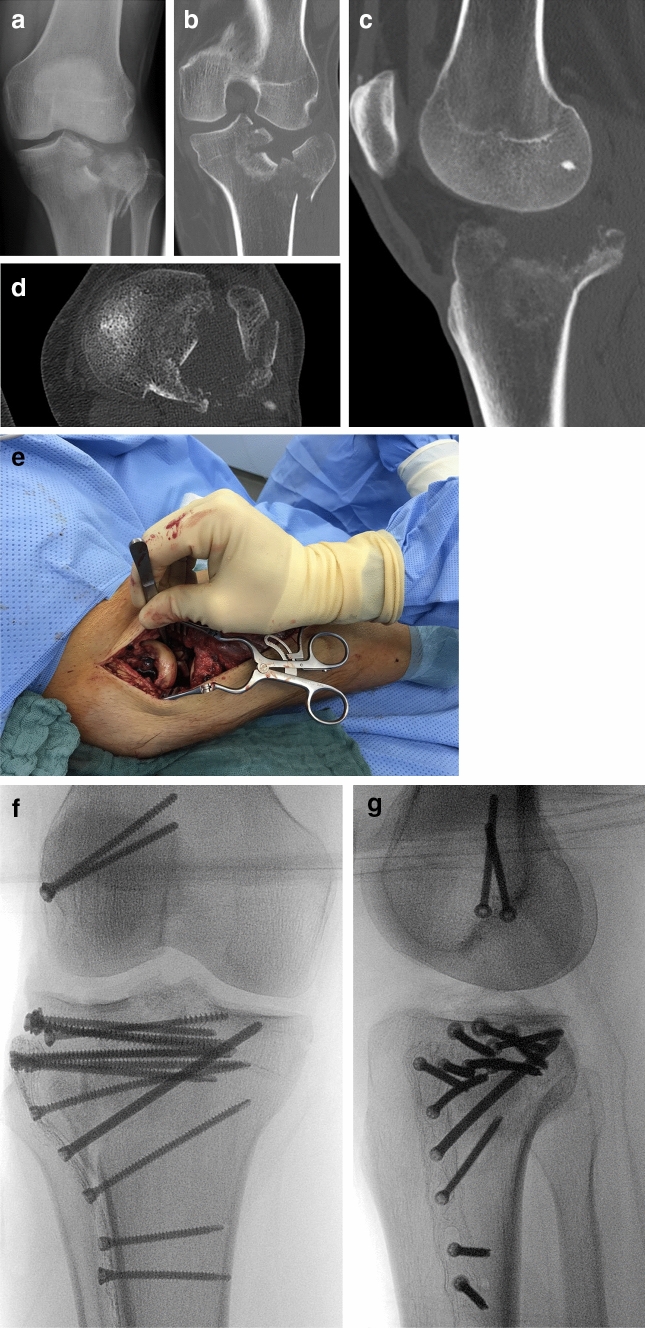
Malreduction after tibial plateau fractures mainly occurs due to insufficient visualization of the articular surface. In 85% of all C-type fractures an involvement of the posterolateral-central segment is observed, which is the main region of malreduction. The choice of the approach is determined (1) by the articular area which needs to be visualized and (2) the positioning of the fixation material. For simple lateral plateau fractures without involvement of the posterolateral-central segment an anterolateral standard approach in supine position with a lateral plating is the treatment of choice in most cases. For complex fractures the surgeon has to consider, that the articular surface of the lateral plateau only can be completely visualized by extended approaches in supine, lateral and prone position. Anterolateral and lateral plating can also be performed in supine, lateral and prone position. A direct fixation of the posterolateral-central segment by a plate or a screw from posterior can be only achieved in prone or lateral position, not supine. The posterolateral approach includes the use of two windows for direct visualization of the fracture. If visualization is insufficient the approach can be extended by lateral epicondylar osteotomy which allows exposure of at least 83% of the lateral articular surface. Additional central subluxation of the lateral meniscus allows to expose almost 100% of the articular surface. The concept of stepwise extension of the approach is helpful and should be individually performed as needed to achieve anatomic reduction and stable fixation of tibial plateau fractures.
Keywords: Anatomic reduction; Osteosynthesis; Posterolateral corner; Surgical approach; Tibial plateau fracture.
Conflict of interest statement
KH Frosch received royalties and fees for presentations from Arthrex. All other authors have no conflicts of interest.
Figures
References
-
- Parkkinen M, Madanat R, Mustonen A, Koskinen S, Paavola M, Lindahl J. Factors predicting the development of early osteoarthritis following lateral tibial plateau fractures: mid-term clinical and radiographic outcomes of 73 operatively treated patients. Scand J Surg. 2014;103(4):256–262. doi: 10.1177/1457496914520854. - DOI - PubMed
-
- Honkonen SE. Indications for surgical treatment of tibial condyle fractures. Clin Orthop Relat Res. 1994;302:199–205. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
