

Association of Bempedoic Acid Administration With Atherogenic Lipid Levels in Phase 3 Randomized Clinical Trials of Patients With Hypercholesterolemia
- PMID: 32609313
- PMCID: PMC7330832
- DOI: 10.1001/jamacardio.2020.2314
Association of Bempedoic Acid Administration With Atherogenic Lipid Levels in Phase 3 Randomized Clinical Trials of Patients With Hypercholesterolemia
Abstract
Importance: Additional lipid-lowering therapy options are needed for patients who cannot achieve sufficient decreases in low-density lipoprotein cholesterol (LDL-C) levels using statins alone or for those who are statin intolerant.
Objective: To conduct a pooled analysis of phase 3 randomized clinical trials of bempedoic acid vs placebo.
Design, setting, and participants: This analysis pooled data from 4 double-blind, placebo-controlled randomized clinical trials conducted from 2016 to 2018. Patients were enrolled in North America and Europe. Eligibility criteria included hypercholesterolemia while receiving stable lipid-lowering therapy and high cardiovascular risk or hypercholesterolemia and statin intolerance.
Interventions: Patients were randomized 2:1 to bempedoic acid, 180 mg (n = 2425), or placebo (n = 1198) once daily for 12 to 52 weeks.
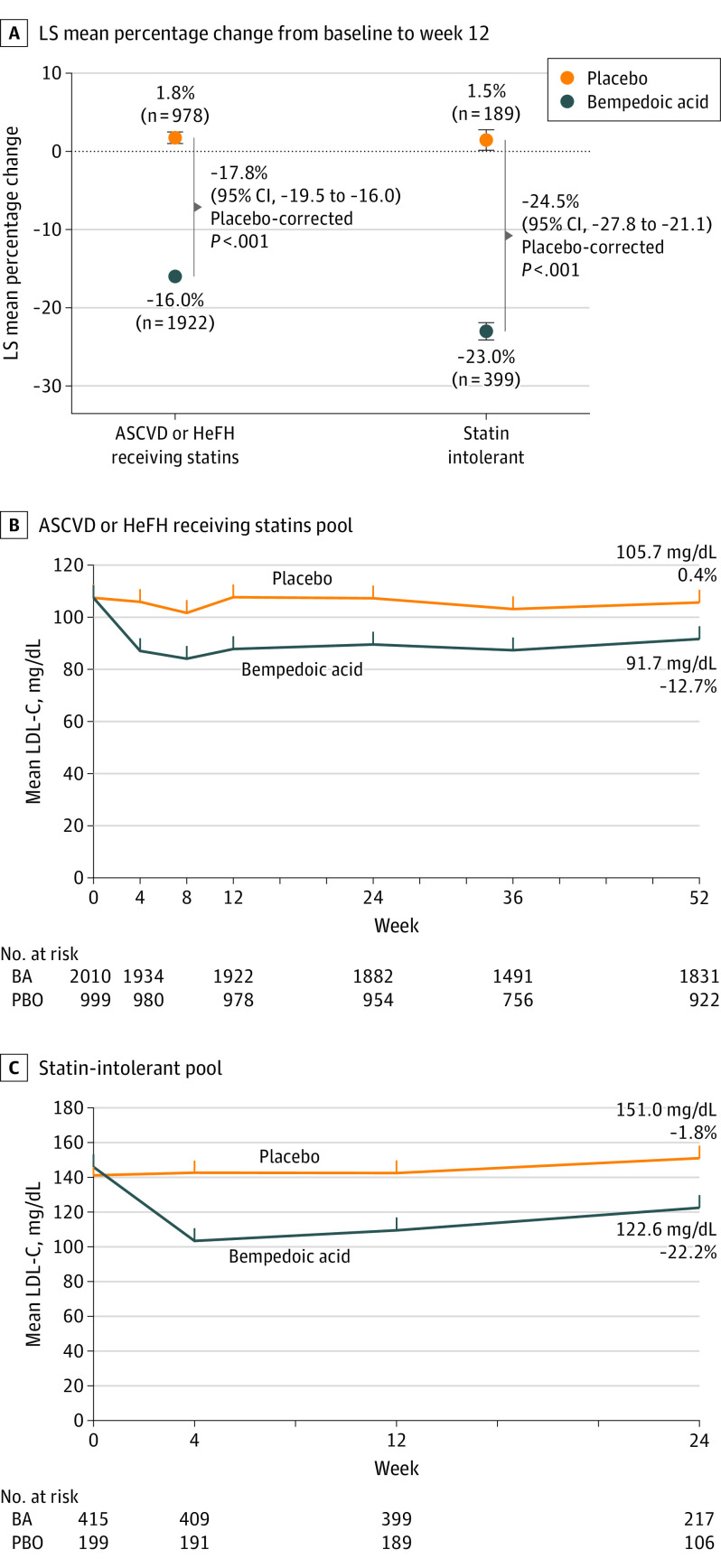
Main outcomes and measures: Primary efficacy end point was percentage change from baseline in LDL-C level at week 12 in the intention-to-treat population. Patients were parsed into 2 groups according to enrollment criteria: (1) patients with hypercholesterolemia and atherosclerotic cardiovascular disease (ASCVD) or with heterozygous familial hypercholesterolemia (HeFH) or with both and receiving statins and (2) patients with hypercholesterolemia who were statin intolerant receiving maximally tolerated statins.
Results: In this analysis of 3623 patients, the overall mean (SD) patient age was 65.5 (9.2) years (similar in both pools). Among patients with ASCVD or HeFH or both, the mean (SD) baseline LDL-C level was 107.6 (32.7) mg/dL. At week 12, the LDL-C level percentage change from baseline was -16.0% with bempedoic acid vs 1.8% with placebo (difference, -17.8%; 95% CI, -19.5% to -16.0%; P < .001). Patients with statin intolerance had a mean (SD) baseline LDL-C level of 144.4 (38.8) mg/dL. The percentage changes in LDL-C levels at week 12 were -23.0% in the bempedoic acid group and 1.5% in the placebo group (difference, -24.5%; 95% CI, -27.8% to -21.1%; P < .001). The decrease in LDL-C levels with bempedoic acid was sustained during long-term follow-up in both pools (patients with ASCVD or HeFH or both receiving a maximally tolerated statin, difference of -12.7% at week 52; patients with statin intolerance, difference of -22.2% at week 24). Decreases in non-high-density lipoprotein cholesterol, total cholesterol, apolipoprotein B, and high-sensitivity C-reactive protein levels were greater with bempedoic acid vs placebo. Treatment-emergent adverse events associated more frequently with bempedoic acid than with placebo included increased blood uric acid level (2.1% vs 0.5%), gout (1.4% vs 0.4%), decreased glomerular filtration rate (0.7% vs <0.1%), and increased levels of hepatic enzymes (2.8% vs 1.3%).
Conclusions and relevance: Bempedoic acid added to maximally tolerated statins, including moderate- or high-intensity statins or no background statin, was associated with decreased LDL-C levels vs placebo in patients with hypercholesterolemia with an acceptable safety profile. As a nonstatin adjunct or statin alternative, bempedoic acid has potential for use in a broad spectrum of patients.
Trial registration: ClinicalTrials.gov Identifiers: NCT02666664, NCT02991118, NCT03001076, and NCT02988115.
Conflict of interest statement
Figures
References
-
- Baigent C, Blackwell L, Emberson J, et al. ; Cholesterol Treatment Trialists’ (CTT) Collaboration . Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670-1681. doi:10.1016/S0140-6736(10)61350-5 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
