

Assessment of Community Interventions for Bystander Cardiopulmonary Resuscitation in Out-of-Hospital Cardiac Arrest: A Systematic Review and Meta-analysis
- PMID: 32609351
- PMCID: PMC7330721
- DOI: 10.1001/jamanetworkopen.2020.9256
Assessment of Community Interventions for Bystander Cardiopulmonary Resuscitation in Out-of-Hospital Cardiac Arrest: A Systematic Review and Meta-analysis
Abstract
Importance: Outcomes from out-of-hospital cardiac arrests (OHCAs) remain poor. Outcomes associated with community interventions that address bystander cardiopulmonary resuscitation (CPR) remain unclear and need further study.
Objective: To examine community interventions and their association with bystander CPR and survival after OHCA.
Data sources: Literature search of the MEDLINE, Embase, and the Cochrane Library databases from database inception to December 31, 2018, was conducted. Key search terms included cardiopulmonary resuscitation, layperson, basic life support, education, cardiac arrest, and survival.
Study selection: Community intervention studies that reported on comparisons with control and differences in survival following OHCA were included. Studies that focused only on in-hospital interventions, patients with in-hospital cardiac arrest, only dispatcher-assisted CPR, or provision of automated external defibrillators were excluded.
Data extraction and synthesis: Pooled odds ratios (ORs) and 95% CIs were estimated using a random-effects model. This study followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline.
Main outcomes and measures: Thirty-day survival or survival to hospital discharge and bystander CPR rate.
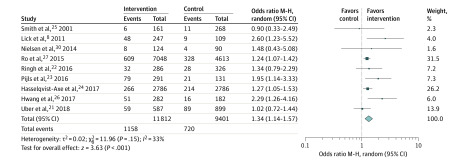
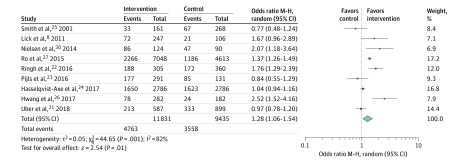
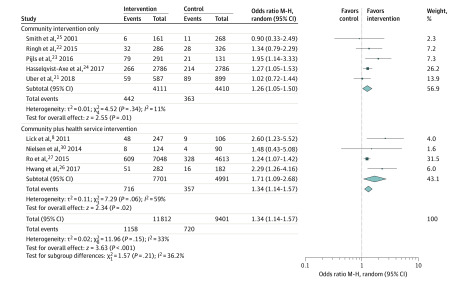
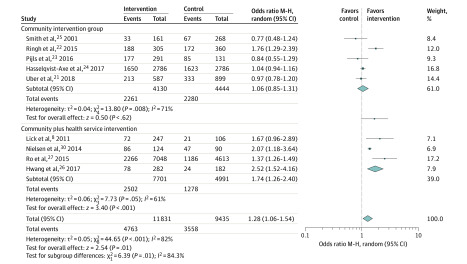
Results: A total of 4480 articles were identified; of these, 15 studies were included for analysis. There were broadly 2 types of interventions: community intervention alone (5 studies) and community intervention combined with changes in health services (10 studies). Four studies involved notification systems that alerted trained lay bystanders to the location of the OHCA in addition to CPR skills training. Meta-analysis of 9 studies including 21 266 patients with OHCA found that community interventions were associated with increased survival to discharge or 30-day survival (OR, 1.34; 95% CI, 1.14-1.57; I2 = 33%) and greater bystander CPR rate (OR, 1.28; 95% CI, 1.06-1.54; I2 = 82%). Compared with community intervention alone, community plus health service intervention was associated with a greater bystander CPR rate compared with community alone (community plus intervention: OR, 1.74; 95% CI, 1.26-2.40 vs community alone: OR, 1.06; 95% CI, 0.85-1.31) (P = .01). Survival rate, however, was not significantly different between intervention types: community plus health service intervention OR, 1.71; 95% CI, 1.09-2.68 vs community only OR, 1.26; 95% CI, 1.05-1.50 (P = .21).
Conclusions and relevance: In this study, while the evidence base is limited, community-based interventions with a focus on improving bystander CPR appeared to be associated with improved survival following OHCA. Further evaluations in diverse settings are needed to enable widespread implementation of such interventions.
Conflict of interest statement
Figures
References
-
- Gräsner JT, Lefering R, Koster RW, et al. ; EuReCa ONE Collaborators . EuReCa ONE-27 Nations, ONE Europe, ONE Registry: a prospective one month analysis of out-of-hospital cardiac arrest outcomes in 27 countries in Europe. Resuscitation. 2016;105:188-195. - PubMed
-
- Benjamin EJ, Virani SS, Callaway CW, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics—2018 update: a report from the American Heart Association. Circulation. 2018;137(12):e67-e492. doi:10.1161/CIR.0000000000000558 - DOI - PubMed
-
- Beck B, Bray J, Cameron P, et al. ; Aus-ROC Steering Committee . Regional variation in the characteristics, incidence and outcomes of out-of-hospital cardiac arrest in Australia and New Zealand: results from the Aus-ROC Epistry. Resuscitation. 2018;126:49-57. doi:10.1016/j.resuscitation.2018.02.029 - DOI - PubMed
