

Plant-Dominant Low-Protein Diet for Conservative Management of Chronic Kidney Disease
- PMID: 32610641
- PMCID: PMC7400005
- DOI: 10.3390/nu12071931
Plant-Dominant Low-Protein Diet for Conservative Management of Chronic Kidney Disease
Abstract
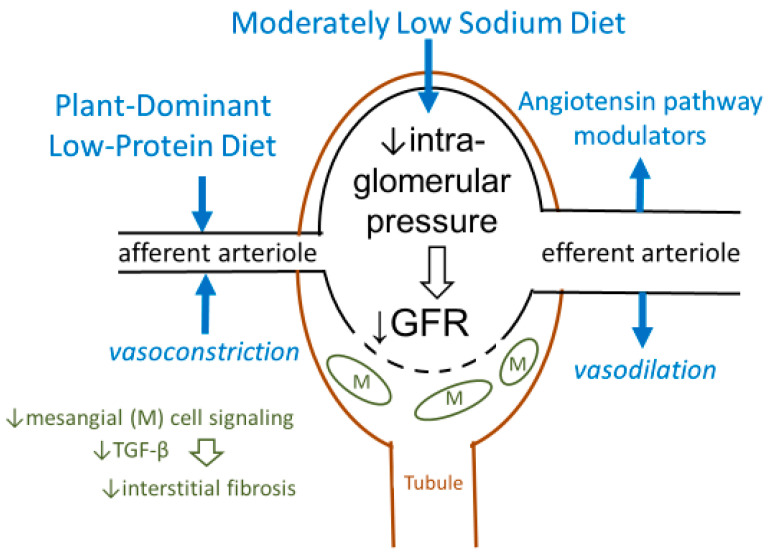
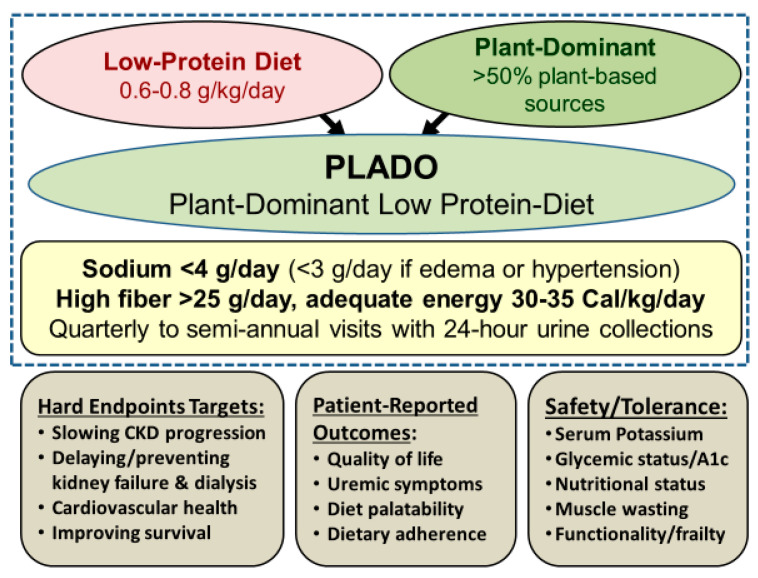
Chronic kidney disease (CKD) affects >10% of the adult population. Each year, approximately 120,000 Americans develop end-stage kidney disease and initiate dialysis, which is costly and associated with functional impairments, worse health-related quality of life, and high early-mortality rates, exceeding 20% in the first year. Recent declarations by the World Kidney Day and the U.S. Government Executive Order seek to implement strategies that reduce the burden of kidney failure by slowing CKD progression and controlling uremia without dialysis. Pragmatic dietary interventions may have a role in improving CKD outcomes and preventing or delaying dialysis initiation. Evidence suggests that a patient-centered plant-dominant low-protein diet (PLADO) of 0.6–0.8 g/kg/day composed of >50% plant-based sources, administered by dietitians trained in non-dialysis CKD care, is promising and consistent with the precision nutrition. The scientific premise of the PLADO stems from the observations that high protein diets with high meat intake not only result in higher cardiovascular disease risk but also higher CKD incidence and faster CKD progression due to increased intraglomerular pressure and glomerular hyperfiltration. Meat intake increases production of nitrogenous end-products, worsens uremia, and may increase the risk of constipation with resulting hyperkalemia from the typical low fiber intake. A plant-dominant, fiber-rich, low-protein diet may lead to favorable alterations in the gut microbiome, which can modulate uremic toxin generation and slow CKD progression, along with reducing cardiovascular risk. PLADO is a heart-healthy, safe, flexible, and feasible diet that could be the centerpiece of a conservative and preservative CKD-management strategy that challenges the prevailing dialysis-centered paradigm.
Keywords: plant-dominant; low-protein; dietary protein intake; glomerular hyperfiltration.
Conflict of interest statement
K. Kalantar-Zadeh has received honoraria and/or support from Abbott, Abbvie, ACI Clinical (Cara Therapeutics), Akebia, Alexion, Amgen, Ardelyx, ASN (American Society of Nephrology), Astra-Zeneca, Aveo, BBraun, Chugai, Cytokinetics, Daiichi, DaVita, Fresenius, Genentech, Haymarket Media, Hofstra Medical School, IFKF (International Federation of Kidney Foundations), ISH (International Society of Hemodialysis), International Society of Renal Nutrition & Metabolism (ISRNM), JSDT (Japanese Society of Dialysis Therapy), Hospira, Kabi, Keryx, Kissei, Novartis, OPKO, NIH (National Institutes of Health), NKF (National Kidney Foundations), Pfizer, Regulus, Relypsa, Resverlogix, Dr Schaer, Sandoz, Sanofi, Shire, VA (Veterans’ Affairs), Vifor, UpToDate, ZS-Pharma. No relevant sources of conflict of interest have been declared by other authors.
Figures
References
-
- Li P.K., Garcia-Garcia G., Lui S.F., Andreoli S., Fung W.W., Hradsky A., Kumaraswami L., Liakopoulos V., Rakhimova Z., Saadi G., et al. Kidney health for everyone everywhere-from prevention to detection and equitable access to care. Kidney Int. 2020;97:226–232. doi: 10.1016/j.kint.2019.12.002. - DOI - PubMed
-
- Kalantar-Zadeh K., Crowley S.T., Beddhu S., Chen J.L.T., Daugirdas J.T., Goldfarb D.S., Jin A., Kovesdy C.P., Leehey D.J., Moradi H., et al. Renal Replacement Therapy and Incremental Hemodialysis for Veterans with Advanced Chronic Kidney Disease. Semin. Dial. 2017;30:251–261. doi: 10.1111/sdi.12601. - DOI - PMC - PubMed
-
- Kalantar-Zadeh K., Moore L.W., Tortorici A.R., Chou J.A., St-Jules D.E., Aoun A., Rojas-Bautista V., Tschida A.K., Rhee C.M., Shah A.A., et al. North American experience with Low protein diet for Non-dialysis-dependent chronic kidney disease. BMC Nephrol. 2016;17:90. doi: 10.1186/s12882-016-0304-9. - DOI - PMC - PubMed
-
- Saran R., Shahinian V., Pearsonm A., Tilea A., Steffick D., Wyncott A., Bragg-Gresham J., Heung M., Morgenstern M., Hutton D., et al. Establishing a National Population Health Management System for Kidney Disease: The Veterans Health Administration Renal Information System (VA-REINS) Am. J. Kidney Dis. 2017;5:A3.
-
- Saran R., Li Y., Robinson B., Abbott K.C., Agodoa L.Y., Ayanian J., Bragg-Gresham J., Balkrishnan R., Chen J.L., Cope E., et al. US Renal Data System 2015 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2016;67(Suppl. 1):S1–S305. doi: 10.1053/j.ajkd.2015.12.014. - DOI - PMC - PubMed
