

Oral Surgical Management of Bone and Soft Tissues in MRONJ Treatment: A Decisional Tree
- PMID: 32610675
- PMCID: PMC7399969
- DOI: 10.3390/life10070099
Oral Surgical Management of Bone and Soft Tissues in MRONJ Treatment: A Decisional Tree
Abstract
Background: The aim of the present work was to analyze a 10-year retrospective series of surgically treated medication-related osteonecrosis of the jaws (MRONJ) cases, reporting the clinical outcome and success rate for each adopted procedure in order to draw a treatment algorithm that is able to standardize clinical decision making and maximize the success of oral surgical treatment of MRONJ.
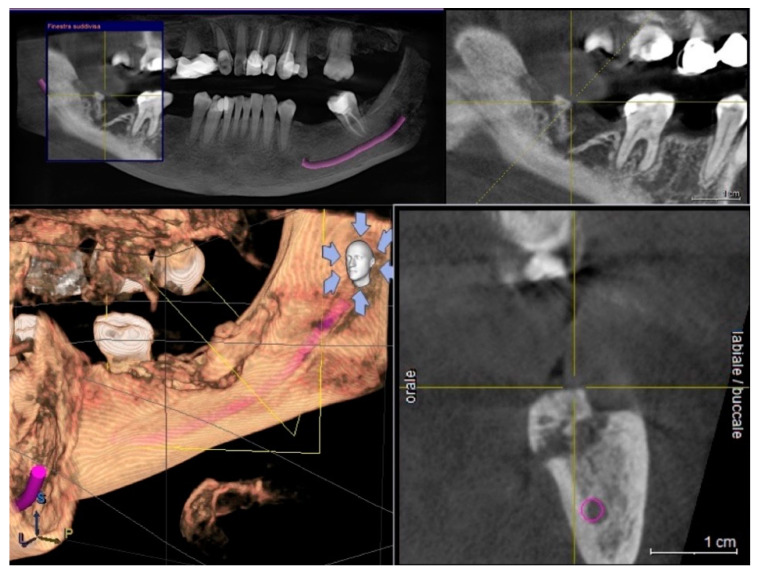
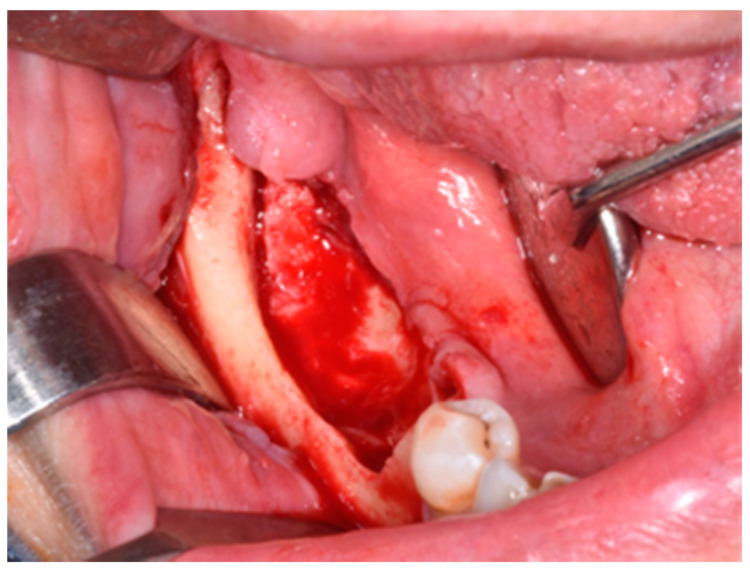
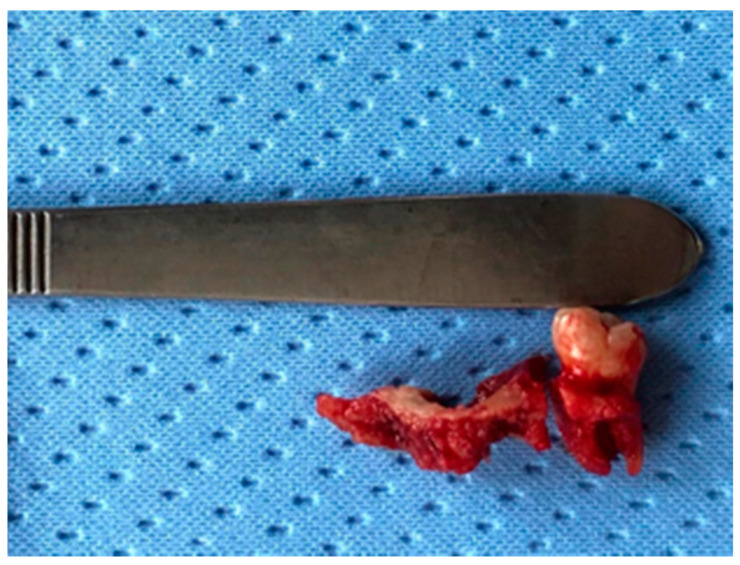
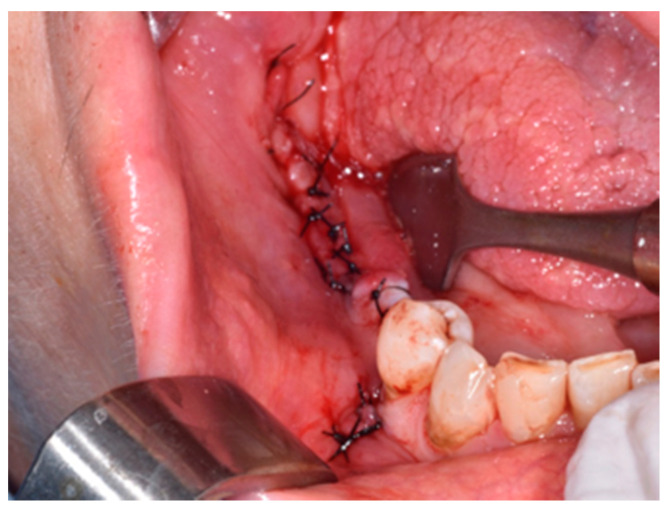
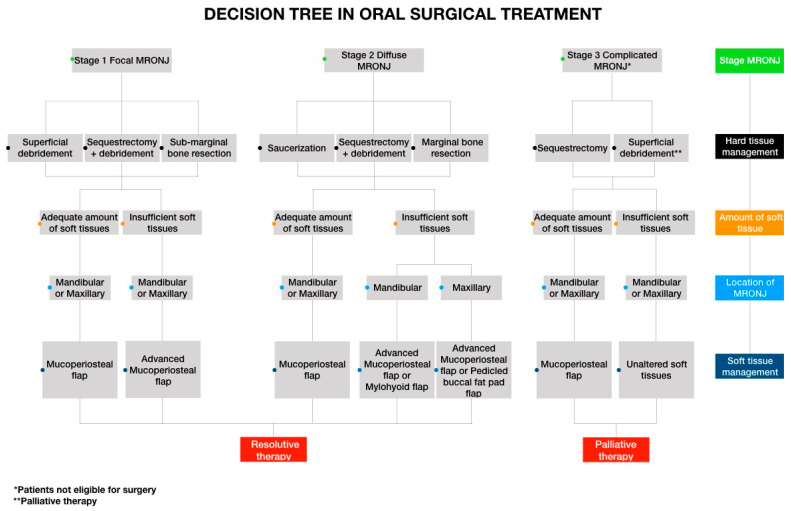
Methods: Different surgical approaches were categorized taking into consideration two variables a) hard tissue management (defined as debridement, saucerization or marginal resective surgery of maxillary necrotic bone) and b) soft tissue management (defined as type of flap design and related modality of wound-healing).
Results: For the retrospective cohort study, 103 MRONJ patients were enrolled and a total of 128 surgical procedures were performed. The role of radical-intended surgery using local flaps in MRONJ treatment was investigated, as well as palliative treatments. All stage I-II patients completely healed when a combination of radical necrotic bone surgery associated with a first intention healing of soft tissues was obtained. In stage III, when a patient was not eligible for maxillo-facial surgery, the use of palliative surgical strategies was effective in symptom relief in order to maintain a better quality of life for the duration of the patient's life.
Conclusions: Oral surgery with radical intent associated with a flap design able to ensure first intention healing might represent a valid option for the majority of MRONJ patients. The designed decision tree allows clinicians to assess individual surgical approaches for MRONJ treatment in accordance with patient-centered outcomes and surgical skills.
Keywords: MRONJ management; MRONJ surgical treatment; oral flaps; reconstructive surgery.
Conflict of interest statement
The authors declare no conflict of interest.
Figures






References
-
- Yoneda T., Hagino H., Sugimoto T., Ohta H., Takahashi S., Soen S., Taguchi A., Nagata T., Urade M., Shibahara T., et al. Antiresorptive agent-related osteonecrosis of the jaw: Position paper 2017 of the Japanese allied committee on osteonecrosis of the jaw. J. Bone Miner. Metab. 2016;35:6–19. doi: 10.1007/s00774-016-0810-7. - DOI - PubMed
-
- Kim H.Y., Lee S.-J., Kim S.-M., Myoung H., Hwang S.J., Choi J.-Y., Lee J.-H., Choung P.-H., Kim M.-J., Seo B.-M. Extensive surgical procedures result in better treatment outcomes for bisphosphonate-related osteonecrosis of the jaw in patients with osteoporosis. J. Oral Maxillofac. Surg. 2017;75:1404–1413. doi: 10.1016/j.joms.2016.12.014. - DOI - PubMed
-
- Yarom N., Shapiro C.L., Peterson D.E., Van Poznak C.H., Bohlke K., Ruggiero S.L., Migliorati C.A., Khan A., Morrison A., Anderson H., et al. Medication-related osteonecrosis of the jaw: MASCC/ISOO/ASCO clinical practice guideline. J. Clin. Oncol. 2019;37:2270–2290. doi: 10.1200/JCO.19.01186. - DOI - PubMed
-
- Wilde F., Heufelder M., Winter K., Hendricks J., Frerich B., Schramm A., Hemprich A. The role of surgical therapy in the management of intravenous bisphosphonates-related osteonecrosis of the jaw. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011;111:153–163. doi: 10.1016/j.tripleo.2010.04.015. - DOI - PubMed
LinkOut - more resources
Full Text Sources
