

Interrelationships between symptom burden and health functioning and health care utilization among veterans with persistent physical symptoms
- PMID: 32611312
- PMCID: PMC7329405
- DOI: 10.1186/s12875-020-01193-y
Interrelationships between symptom burden and health functioning and health care utilization among veterans with persistent physical symptoms
Abstract
Background: Between 10 and 50% of primary care patients present with persistent physical symptoms (PPS). Patients with PPS tend to utilize excessive or inappropriate health care services, while being stuck in a deleterious cycle of inactivity, deconditioning, and further worsening of symptoms and disability. Since military deployment (relative to non-deployment) is associated with greater likelihood of PPS, we examined the interrelationships of health care utilization, symptom burden and functioning among a sample of recently deployed Veterans with new onset persistent physical symptoms.
Methods: This study analyzed a cohort of 790 U.S. soldiers who recently returned from deployment to Iraq or Afghanistan. Data for this analysis were obtained at pre- and post-deployment. We used moderation analyses to evaluate interactions between physical symptom burden and physical and mental health functioning and four types of health care utilization one-year after deployment, after adjusting for key baseline measures.
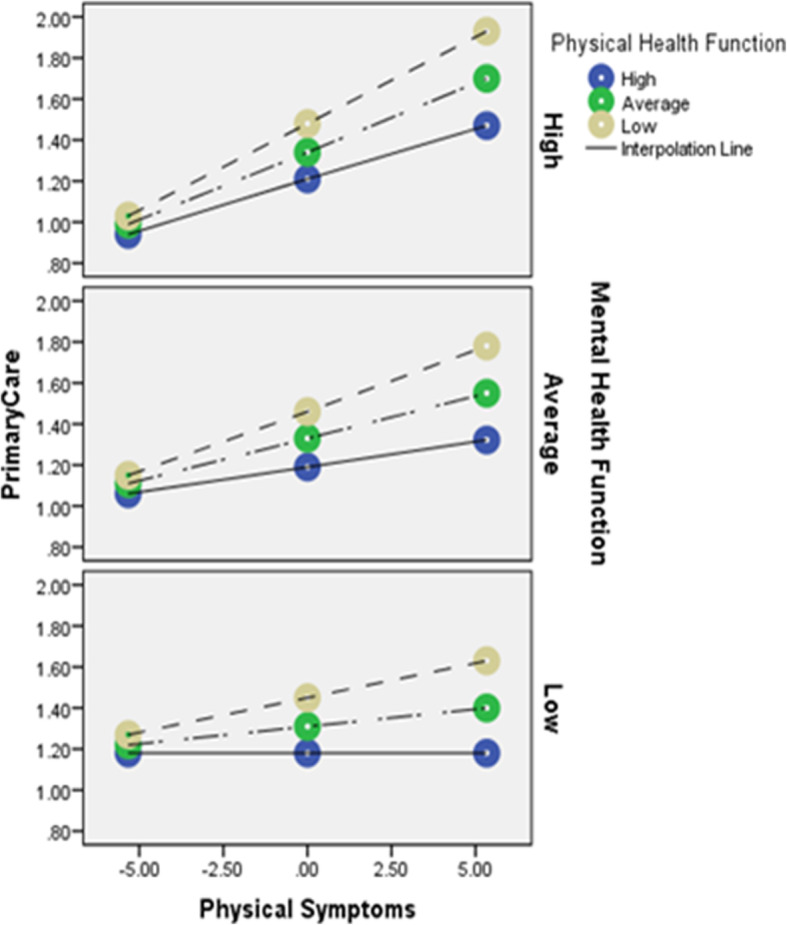
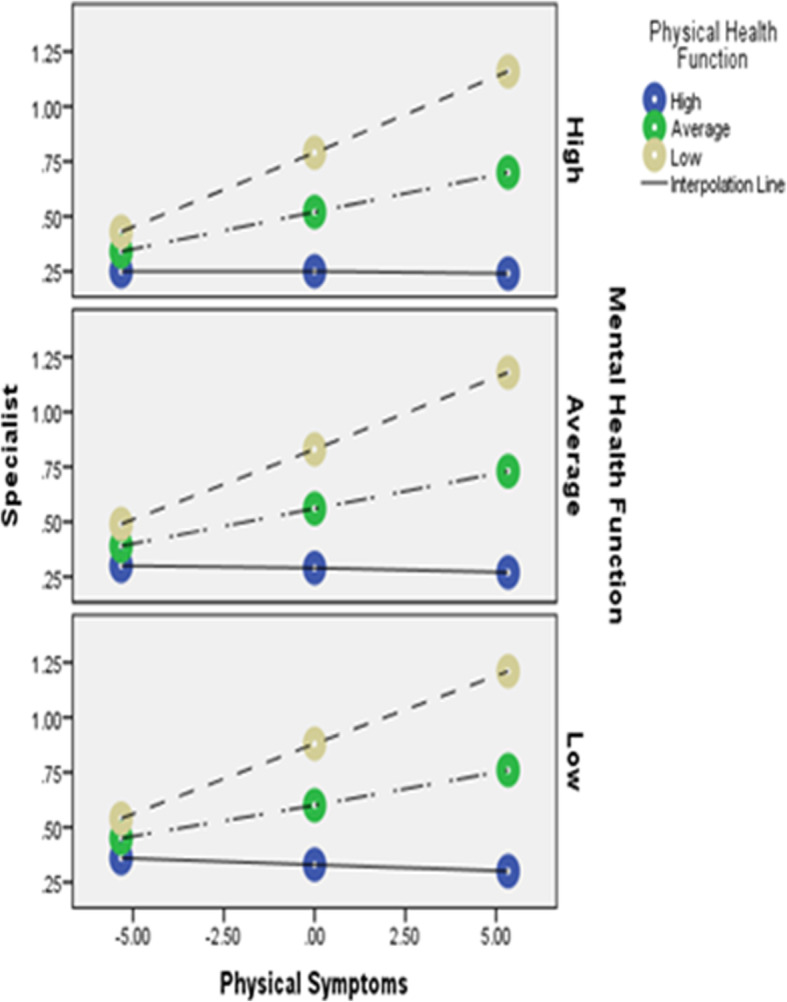
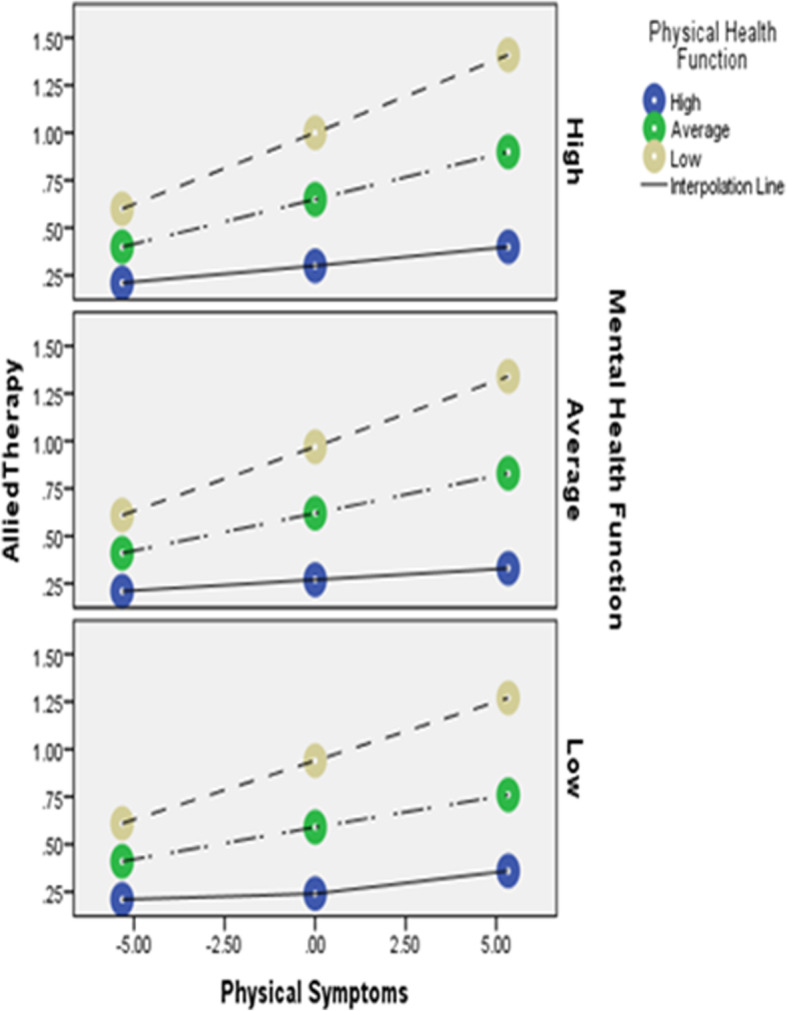
Results: Moderation analyses revealed significant triple interactions between physical symptom burden and health functioning and: primary care (F = 3.63 [2, 303], R2Δ = .02, p = 0.03), specialty care (F = 6.81 [2, 303] R2Δ =0.03, p < .001), allied therapy care (F = 3.76 [2, 302], R2Δ = .02, p = 0.02), but not mental health care (F = 1.82 [1, 303], R2Δ = .01, p = .16), one-year after deployment.
Conclusions: Among U.S. Veterans with newly emerging persistent physical symptoms one-year after deployment, increased physical symptom burden coupled with decreased physical and increased mental health functioning was associated with increased medical care use in the year after deployment. These findings support whole health initiatives aimed at improving health function/well-being, rather than merely symptom alleviation.
Keywords: Health care utilization; Health functioning; Medically unexplained symptoms; Persistent physical symptoms; Symptoms; Veterans.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
The overlooked burden of persistent physical symptoms: a call for action in European healthcare.Lancet Reg Health Eur. 2024 Nov 26;48:101140. doi: 10.1016/j.lanepe.2024.101140. eCollection 2025 Jan. Lancet Reg Health Eur. 2024. PMID: 39660101 Free PMC article. Review.
-
High healthcare utilization near the onset of medically unexplained symptoms.J Psychosom Res. 2017 Jul;98:98-105. doi: 10.1016/j.jpsychores.2017.05.001. Epub 2017 May 3. J Psychosom Res. 2017. PMID: 28554378
-
Mental health problems, use of mental health services, and attrition from military service after returning from deployment to Iraq or Afghanistan.JAMA. 2006 Mar 1;295(9):1023-32. doi: 10.1001/jama.295.9.1023. JAMA. 2006. PMID: 16507803
-
Psychosocial Functioning and Health-Related Quality of Life Associated with Posttraumatic Stress Disorder in Male and Female Iraq and Afghanistan War Veterans: The VALOR Registry.J Womens Health (Larchmt). 2015 Dec;24(12):1038-46. doi: 10.1089/jwh.2014.5096. Epub 2015 Jul 23. J Womens Health (Larchmt). 2015. PMID: 26204466
-
Functional Somatic Symptoms.Dtsch Arztebl Int. 2019 Aug 9;116(33-34):553-560. doi: 10.3238/arztebl.2019.0553. Dtsch Arztebl Int. 2019. PMID: 31554544 Free PMC article.
Cited by
-
Inequity in the healthcare utilization among latent classes of elderly people with chronic diseases and decomposition analysis in China.BMC Geriatr. 2022 Nov 11;22(1):846. doi: 10.1186/s12877-022-03538-x. BMC Geriatr. 2022. PMID: 36357825 Free PMC article.
-
The overlooked burden of persistent physical symptoms: a call for action in European healthcare.Lancet Reg Health Eur. 2024 Nov 26;48:101140. doi: 10.1016/j.lanepe.2024.101140. eCollection 2025 Jan. Lancet Reg Health Eur. 2024. PMID: 39660101 Free PMC article. Review.
References
-
- Isaac ML, Paauw DS. Medically unexplained symptoms. Med Clin. 2014;98(3):663–672. - PubMed
-
- Salmon P, Humphris GM, Ring A, Davies JC, Dowrick CF. Why do primary care physicians propose medical care to patients with medically unexplained symptoms? A new method of sequence analysis to test theories of patient pressure. Psychosom Med. 2006;68(4):570–577. doi: 10.1097/01.psy.0000227690.95757.64. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
