

Association of guideline publication and delays to treatment in pediatric status epilepticus
- PMID: 32611646
- PMCID: PMC7538224
- DOI: 10.1212/WNL.0000000000010174
Association of guideline publication and delays to treatment in pediatric status epilepticus
Abstract
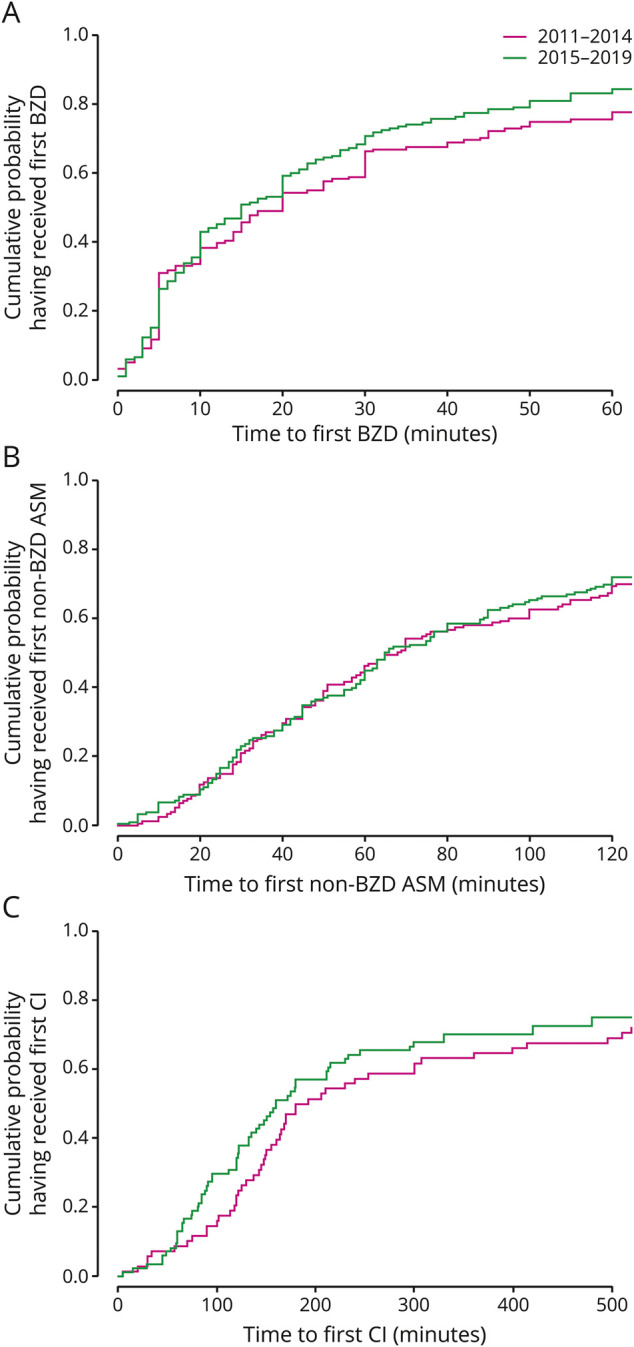
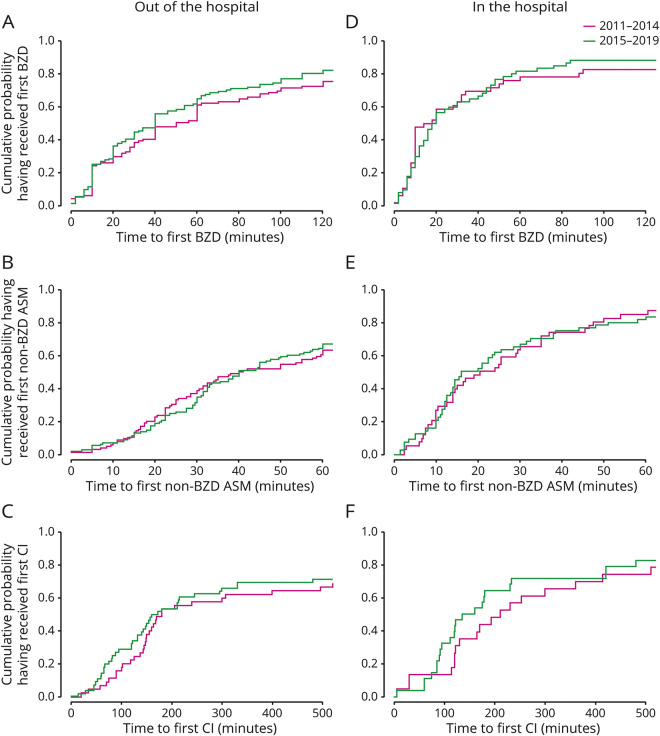
Objective: To determine whether publication of evidence on delays in time to treatment shortens time to treatment in pediatric refractory convulsive status epilepticus (rSE), we compared time to treatment before (2011-2014) and after (2015-2019) publication of evidence of delays in treatment of rSE in the Pediatric Status Epilepticus Research Group (pSERG) as assessed by patient interviews and record review.
Methods: We performed a retrospective analysis of a prospectively collected dataset from June 2011 to September 2019 on pediatric patients (1 month-21 years of age) with rSE.
Results: We studied 328 patients (56% male) with median (25th-75th percentile [p25-p75]) age of 3.8 (1.3-9.4) years. There were no differences in the median (p25-p75) time to first benzodiazepine (BZD) (20 [5-52.5] vs 15 [5-38] minutes, p = 0.3919), time to first non-BZD antiseizure medication (68 [34.5-163.5] vs 65 [33-142] minutes, p = 0.7328), and time to first continuous infusion (186 [124.2-571] vs 160 [89.5-495] minutes, p = 0.2236). Among 157 patients with out-of-hospital onset whose time to hospital arrival was available, the proportion who received at least 1 BZD before hospital arrival increased after publication of evidence of delays (41 of 81 [50.6%] vs 57 of 76 [75%], p = 0.0018), and the odds ratio (OR) was also increased in multivariable logistic regression (OR 4.35 [95% confidence interval 1.96-10.3], p = 0.0005).
Conclusion: Publication of evidence on delays in time to treatment was not associated with improvements in time to treatment of rSE, although it was associated with an increase in the proportion of patients who received at least 1 BZD before hospital arrival.
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
Comment in
-
Reader Response: Association of Guideline Publication and Delays to Treatment in Pediatric Status Epilepticus.Neurology. 2021 Mar 9;96(10):502-503. doi: 10.1212/WNL.0000000000011561. Neurology. 2021. PMID: 33686007 No abstract available.
-
Author Response: Association of Guideline Publication and Delays to Treatment in Pediatric Status Epilepticus.Neurology. 2021 Mar 9;96(10):503. doi: 10.1212/WNL.0000000000011560. Neurology. 2021. PMID: 33686008 No abstract available.
References
-
- Chin RF, Neville BG, Peckham C, et al. Incidence, cause, and short-term outcome of convulsive status epilepticus in childhood: prospective population-based study. Lancet 2006;368:222–229. - PubMed
-
- Coeytaux A, Jallon P, Galobardes B, Morabia A. Incidence of status epilepticus in French-speaking Switzerland (EPISTAR). Neurology 2000;55:693–697. - PubMed
-
- Dham BS, Hunter K, Rincon F. The epidemiology of status epilepticus in the United States. Neurocrit Care 2014;20:476–483. - PubMed
-
- Wu YW, Shek DW, Garcia PA, Zhao S, Johnston SC. Incidence and mortality of generalized convulsive status epilepticus in California. Neurology 2002;58:1070–1076. - PubMed
-
- Sánchez Fernández I, Loddenkemper T. Estimating the cost of admissions related to convulsive status epilepticus in the United States of America. Seizure 2018;61:186–198. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical